
Rulide
| Contato
Página Inicial
Professor J?rgen Floege
- Professor of Nephrology
- Division of Nephrology
- University Hospital
- Aachen
- Germany
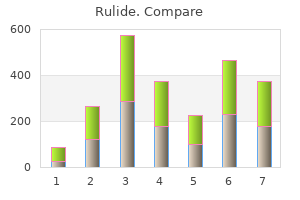
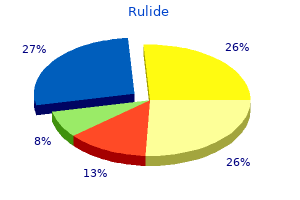
The Sprint Fidelis advisory is again highlighted as a prime example of the failure of our current surveillance systems medications safe while breastfeeding purchase genuine rulide online. At present there is no international standard addressing the appropriate management of advisory situations symptoms ear infection order rulide 150mg line. Each advisory presents a unique set of circumstances treatment 1st degree heart block generic rulide 150mg on line, which makes the creation of universal guidelines beyond overarching principles a significant challenge treatment yellow tongue purchase 150 mg rulide mastercard. Looking forward symptoms 5 days before your missed period buy rulide canada, a key goal would be the creation of an international network of active surveillance and reporting not only to facilitate the identification of advisory situations, but also to promote a unified approach to management. Advisory devices and leads can be associated with substantial risk of complications including death, a key consideration in the development of guidelines in this area. Schellenberg G, Turcotte M: A portrait of seniors in Canada, 2006, Statistics Canada. Cuvillier E: Handbook of leads for pacing, defibrillation, & cardiac resynchronization, ed 2, 2011, Massachusetts Medical Society. Auricchio A, Gropp M, Ludgate S, et al: European Heart Rhythm Association guidance document on cardiac rhythm management product performance. Lakkireddy D, Valasareddi S, Ryschon K, et al: the impact of povidone-iodine pocket irrigation use on pacemaker and defibrillator infections. Yee R, Verma A, Beardsall M, et al: Canadian Cardiovascular Society/Canadian Heart Rhythm Society joint position statement on the use of remote monitoring for cardiovascular implantable electronic device follow-up. Li X, Ze F, Wang L, et al: Prevalence of venous occlusion in patients referred for lead extraction: implications for tool selection. Parkash R, Tung S, Champagne J, et al: Insight into the mechanism of failure in the Riata lead under advisory. Urgent Medical Device Information Sprint Fidelis Lead Patient Management Recommendations. Parkash R, Crystal E, Bashir J, et al: Complications associated with revision of Sprint Fidelis leads: report from the Canadian Heart Rhythm Society Device Advisory Committee. Parkash R, Thibault B, Sterns L, et al: the Fidelis lead fracture occurs more frequently in patients with cardiac resynchronization therapy. Visit duration in terms of total cumulative time lasted a mean of 27 minutes for scheduled visits and was about 30% longer for unscheduled visits. Most visits involved the simultaneous use of two different types of health care personnel (239/407, 59%). The most frequent combination included only the involvement of a cardiologist and a nurse (216/407), whereas 65 additional visits also included an internal or external technician or both. Current technology and software platforms allow access to the same data and diagnostics that can be accessed at a face to face visit. In parallel, moving toward disease management implies a substantial increase in the burden of care, with important organizational issues, including a connection with heart failure specialists. In some cases, specialized assessment and counseling should be considered in selected patients. However, storage and retrieval of the data collected remotely and in person is extremely powerful and can greatly improve the efficiency, communication, and assessment of device management. In part, everyone who employs the remote interrogation paradigm is a potential recipient of the advantages of the database approach to follow-up. It is important that the system has the ability to collect both these types of data. Using these standards allows for a reproducible, lower cost, and reliable information system. This multidisciplinary approach is, in effect, a link between clinical evidence and policy making, informing government agencies, health care professionals and administrators, private sector organizations, the healthcare industry, as well as patients, insurance carriers, and the general public. With regard to devices, a wide heterogeneity exists in reimbursement practices across Europe, North America, and Asia. The lack of reimbursement is reported as the most important barrier to full implementation of remote monitoring from around 58% to 72% of centres. In the perspective of the hospital, optimization of the workflow during in-person follow-up, with precise definition of the roles of nurses, technicians, and physicians, coupled with synchronization of their activities can reduce the time spent for in-office checks and lead to better use of human resources. Optimization of device programming should be one of the goals of device clinics in order to save resources. Larsson B, Elmqvist H, Rydén L, Schüller H: Lessons from the first patient with an implanted pacemaker: 1958-2001. Boriani G, Auricchio A, Klersy C, et al: Healthcare personnel resource burden related to in-clinic follow-up of cardiovascular implantable electronic devices: a European Heart Rhythm Association and Eucomed joint survey. Boriani G, Maniadakis N, Auricchio A, et al: Health technology assessment in interventional electrophysiology and device therapy: a position paper of the European Heart Rhythm Association. Braunschweig F, Boriani G, Bauer A, et al: Management of patients receiving implantable cardiac defibrillator shocks: recommendations for acute and long-term patient management. Boriani G, Diemberger I, Biffi M, et al: Cardiac resynchronization therapy in clinical practice: need for electrical, mechanical, clinical and logistic synchronization. Boriani G, Diemberger I, Martignani C, et al: Telecardiology and remote monitoring of implanted electrical devices: the potential for fresh clinical care perspectives. Boriani G: Remote monitoring of cardiac implantable electrical devices in Europe: quo vadis Boriani G, Biffi M, Branzi A, et al: Benefits in projected pacemaker longevity and in pacing related costs conferred by automatic threshold tracking. Burri H, Heidbuchel H, Jung W, Brugada P: Remote monitoring: a cost or an investment In the last several decades, the developing world has witnessed a rapid rise in the cardiovascular disease epidemic, fueled by a combination of rising risk factors, such as hypertension, diabetes mellitus, tobacco use, lack of physical activity, and unhealthy diet. Multiple factors are likely responsible for the observed variations in both surveys; among them are socioeconomic disparities, varied access to health care, and quality of care. The most direct causes of disparity may be variable availability of implanting physicians, health care infrastructure, and device access. In other cases, universal insurance does not cover the high cost of electrophysiologic therapy. It has been estimated that perhaps as many as a million people die each year in the world due to lack of access to pacemaker therapy. A successful large-scale device reuse program would necessitate the coordinated participation of many stakeholders, including the manufacturers, the regulators, and the professional societies. It may enable the surviving family to build an empathetic interconnection with patients who, like their loved ones, suffer from cardiovascular disease (personal communication with donors). There may exist cultural or religious obstacles to accepting a donated device which has been removed from the deceased. My Heart Your Heart surveyed 593 patients and family members at Centro Nacional Cardiologia in Managua, Nicaragua, and Indus General Hospital in Karachi, Pakistan. The vast majority of patients and their family members would accept a reused pacemaker (77%), even knowing that they may carry a higher risk of infection or device failure (56% and 68%, respectively). These respondents were also overwhelmingly in favor of donating their own hypothetical pacemaker postmortem. Respondents with the ability to pay for their own pacemaker, those with excellent health status, and respondents without personal experience with heart disease were less willing to accept a used device. There is published literature from Sweden, Norway, Finland, Holland, Hungary, Romania, Italy, Israel, India, Brazil, Australia, and Canada, which showed safety of pacemaker reuse. There was no significant difference in infection rate between reused and new pacemakers (P = 0. Compared with new pacemaker implantation, however, there was a six-fold increased risk for malfunction in the reuse group (0. This difference was mainly due to abnormalities in set-screws, as well as nonspecific "technical errors," some of them discovered during the implant procedure. Kantharia et al presented their experience with devices explanted from the deceased between 2004 and 2010. No infections or device failures occurred over a mean of 661 days of follow-up (19 to 1827 days). No infectious complications and no identifiable device-related complications occurred, apart from a lead dislodgement and a lead fracture. Appropriate therapy (shocks or antitachycardia pacing) was delivered to 54% of patients. Finally, recent noninferiority study from Nava et al34 in Mexico reported on 603 consecutive patients who received pacemakers from 2000 to 2010. Patients who could not afford new pacemakers were offered refurbished devices (n = 307). A combined end point of unexpected battery depletion, infection, and device malfunction was not different between new and refurbished pacemakers. The North American Society of Pacing and Electrophysiology Policy Conference43 examined the issue of pacemaker reuse in 1985. Based on the examination of the literature available at that time (nearly 2000 patients with refurbished pacemakers) the policy conference concluded that pulse generator reuse was not a risk factor for device infection. According to the Policy Conference "the implantation of a previously used pacemaker should not be considered substandard care. The authors suggested a projected remaining useful lifetime requirement of 5 years. The authors of the document urged that legal and technical criteria be established to remove the impediments to the adoption of this practice as a means of improving cost-efficiency. European Society of Cardiology Policy Conference in 1998 addressed the issue of device reuse in cardiology shortly after the European Union law produced harmonized legislation. Nonetheless, the regulatory issues were never resolved and reuse of single use devices remains off limits in the European Union. Unfortunately, this does not eliminate all regulatory risk and puts the onus of testing and sterilization on the party that is least able to shoulder the burden. Regulations, which would guide and encourage the medical device manufacturers to support international interchange of reprocessed single-use devices, are lacking. The academic center interacts with the Food and Drug Administration to obtain necessary permits for a clinical study and a registry in countries, whose governments expressly approve the initiative as a means of improving the health care of their citizens. If safety and efficacy can be established to the satisfaction of the professional societies and regulatory bodies, further partnerships and models for collaboration can be developed, and the initiative can be scaled up for maximum benefit of the underserved population. A system of notification to the original manufacturer would be required, because the manufacturers are mandated to maintain patient information. A tracking system for donated product should include the new patient information, so that appropriate notification is made in case of an advisory. Would anyone expect the manufacturers to provide educational and technical support Would the manufacturers expose themselves to legal jeopardy by participating in such an initiative The principle of distributive justice is based on socially just allocation of goods in a society. The society has an interest in health of its members, in part so that they may participate fully as citizens. Given the paramount role that good health plays in the well-being of individuals, access to health care is required for a just society. It sustains them as fully participating citizens-normal collaborators and competitors-in all spheres of social life. This leads us to pose a question of what equitable allocation of resources means in a global society One might argue that fair resource allocation requires the most needy get the "best" pacemakers. And if is not practical or possible to create strict equality across countries, should we feel morally and ethically obliged to at least attempt to seek solutions to the disparities in electrophysiologic care A maximum benefit approach to donor kidney allocation promotes stratifying donor organs based on viability and matching them to the predicted survival of intended recipients. It is argued that fewer cumulative life years would be lost by using more viable organs on patients with greater expected survival, and less viable organs in patients with shorter anticipated survival. The failure to initiate measures that would recycle "medical waste" and turn it into life-saving therapy appears to violate the principle of distributive justice. His seminal work, "A Theory of Justice," became a primary text in political philosophy. Second, Social and economic inequalities are to be arranged so that they are both (a) to the greatest benefit of the least advantaged, and (b) attached to offices and positions open to all under conditions of fair equality of opportunity. The principle holds that in order to provide genuine equality of functioning and opportunity, society must give more attention to those with fewer native assets and to those born into the less favorable social positions. It imposes on us the obligation to prevent sickness or death whenever we reasonably can. If an item is unacceptable in the donor country it is also unacceptable as a donation. Are we compelled to either accept or reject all donations falling below the standard of care in the donor country It is understandable that one would be unwilling to accept product donations, which are nonfunctional or hazardous, as this would simply represent "dumping" of waste. Utilitarian principles governing the just distribution of resources are based on the premise of maximum benefit- the greatest good for the greatest number. At hand we have devices that are currently discarded as waste by the majority of the funeral homes and crematories or buried within the corpses in an environmentally unfriendly fashion. We have access to a resource that, with a relatively modest investment of effort and money, could afford a human being an opportunity for improved quality of life or even extend longevity. According to this principle, all human beings are given autonomy over their bodies, which intrinsically belong to them.
Nanopore metagenomics enables rapid clinical diagnosis of bacterial lower respiratory infection medicine 513 order 150 mg rulide mastercard. Rapid metagenomic identification of viral pathogens in clinical samples by real-time nanopore sequencing analysis symptoms west nile virus buy rulide mastercard. A cloud-compatible bioinformatics pipeline for ultrarapid pathogen identification from next-generation sequencing of clinical samples medications ocd 150 mg rulide order overnight delivery. KrakenUniq: Confident and fast metagenomics classification using unique k-mer counts treatment 5th metatarsal shaft fracture order rulide no prescription. Metagenomic next-generation sequencing of samples from pediatric febrile illness in Tororo medications emts can administer 150 mg rulide amex, Uganda. Virome capture sequencing enables sensitive viral diagnosis and comprehensive virome analysis. Nucleic acid sequence-based amplification assays for rapid detection of West Nile and St. In meeting the challenges of a world whose viral pathogens continue to evolve, the practice of neuropathology has benefitted from many of the same technologies transforming clinical care, particularly molecular diagnostics. Neuropathology has also adapted to surgical techniques such as stereotactic needle biopsy, which allows more targeted and limited sampling of nervous system tissues for analysis. The reduced morbidity of needle biopsy compared to open craniotomy, as well as its acceptable sensitivity, allows for a greater medical tolerance in who can undergo brain biopsy to yield diagnostic tissue, a counterweight to the general diminution of tissue analysis that has resulted from advances in clinical diagnostics (see the last section of this chapter) [5,6]. While many aspects of neuropathologic diagnosis have remained constant for decades, the expansion of recognized viral pathogens and pathologies raises significant obstacles to practice, as there are continual needs to educate practitioners with regard to the appearances of newly recognized diseases and to provide them with the updated immunohistochemical and molecular probes enabling diagnosis. These issues are pertinent not only to neuroanatomic practice but also to hospital pathology laboratories serving clinical diagnostics. As a result of economic forces, definitive diagnosis of viral infection at a fluid or tissue level may sometimes only be possible through referral to a center (such as the Centers for Disease Control and Prevention in Atlanta, a state health department, or a specialized academic laboratory) that maintains its diagnostic competency through a relatively robust referral practice employing the necessary specialized reagents. Furthermore, even when departments maintain diagnostic reagents, these may be of limited value; recently, one study showed that common immunohistochemical reagents used to detect a variety of herpes, adeno and polyomaviruses in tissue section had marginal utility overdetection of viral cytopathic effects by routine hematoxylin and eosin (H&E) histology [7]. What are the temporal characteristics and neuroanatomic distribution of the process Is there a characteristic viral inclusion or specific cellular modification that can be recognized histologically If there is no discernable viral cytopathic effect, do reagents exist that can reliably detect viral protein, glycoprotein, or nucleic acid in the tissue section Host factors are critical determinants of neuropathology, and may sometimes result in para-infectious disorders that can be clinically difficult to distinguish from direct viral effects. However, not all inclusions announce their origins: For example, herpes simplex and varicella zoster viruses result in Cowdry type A intranuclear inclusions that cannot be distinguished in isolation but must be interpreted in the context of a larger tissue histology, which in and of itself may sometimes be inadequate for differentiation. The numerous classes and subclasses of arboviruses, such as members of the Flaviviridae. While characteristic inclusions are induced in oligodendroglia (e), infection of astrocytes is typically restricted and results in nuclear atypia without a viral inclusion (f). Furthermore, a single viral species may display a variety of cellular pathologies within the same infectious locus. There may also be significant "histologically occult" viral infection in nervous system tissues adjacent to active inflammatory or necrotizing pathologies. This, of course, raises the critical issue of distinguishing pathogenic infection from putatively harmless latency, evoking another concept in neuropathology and neuropathogenesis: Neurotropism versus neurovirulence. Inflammation, microglial nodules, neuronophagia in spinal cord and brainstem Meningitis; myelitis targeting anterior horn cells; encephalomyelitis; rhombencephalitis. Microglial nodules with variable amounts of perivascular inflammation and neuronophagia; inflammation of nerves (neuritis) and leptomeninges (meningitis) Fetal infection with spectrum of disorders including microcephaly, lissencephaly, agyria, ventriculomegaly, ocular abnormalities; GuillianBarré syndrome and rarely myelitis and meningoencephalitis in adults Meningitis; encephalitis; myelitis; radiculitis; inflammation and necrosis predominantly in brainstem, spinal cord anterior horn, cerebellum, and deep cerebral gray matter 4. The portal of access is an important determinant of neuropathology, as it dictates not only initial neuroanatomic distribution of virus, but also characteristics of the cellular response. In contrast, rabies virus exploits axonal transport mechanisms with trans-synaptic spread; the resulting neuropathology appears relatively mild in contrast to its dire medical consequences, with a paucity of inflammatory features, and tract-related effects that are without relation to vascular structures [17]. Why a neurotropic infection manifests neurovirulence cannot be explained by a single generalized mechanism across viral classes and species. There are numerous products of viral life cycles and variable aspects of host responsiveness that are factors in neurovirulence. However, many viruses lack specific genetic signatures of neurovirulence, and it is likely that the complex interplay between host response and viral invasion determines disease outcome. Inflammatory and apoptotic responses to infection may be protective or harmful, depending on context [19]. As another example, while apoptosis of neurons might generally be considered to be deleterious, the neuropathology of rabies virus provides a clear contradiction to this: Despite evidence of neuronal infection with profound dysregulation of cell function, survival of infected neurons, and not apoptosis, is critical to the fatal outcome of disease [17]. While virally-induced inflammation is typically mononuclear, some agents may induce a prominent polymorphonuclear response, such as seen in early stages of Eastern equine encephalitis [21]. While inflammatory infiltrates are non-specific, the experienced neuropathologist integrates knowledge of clinical presentation, neuroanatomic distribution, and subtleties of inflammatory morphology in guiding the workup. Microglia can accordingly display a variety of morphologies, with amoeboid, ramified, and intermediate appearances; while these appearances are not sufficient to define the multiple functional states in which microglia may exist (these are only discernable by assaying expression of proteins and nucleic acids), morphologic appearances are sometimes the clues to certain pathogens. While inflammatory morphologies are not absolute indicators of the inciting agent, they may be suggestive and aid in appropriate selection of molecular and immunohistochemical tests for pathogen confirmation. Unfortunately, the vast majority of inflammatory responses to virus are histologically non-specific. A thick collar of lymphocytes is present in the subarachnoid (Virchow-Robin) space surrounding a parenchymal blood vessel. The nodule is composed of both elongated and amoeboid microglia; it is unclear what primary pathogen is responsible due to the lack of any characteristic viral cytopathic effect. Universally, in both adult and pediatric patients with acute presentation, brain biopsy has no role in the initial diagnostic assessment of suspected viral encephalitis. Stereotactic, and sometimes open, brain biopsy is considered at variable time points, dependent on the particular guideline. The Infectious Diseases Society of America reserves biopsy for individuals who manifest encephalitis of unknown etiology and who deteriorate neurologically in the face of treatment with acyclovir [24]. Similarly, in resource-limited regions, brain biopsy does not have a role in diagnosis, as with recommendations originating in India and Brazil [25,30]. British recommendations, for pediatric patients, state that stereotactic biopsy might be considered for children in whom no diagnosis (via analysis of fluids) can be achieved within a week, and in particular when there are focal imaging abnormalities [27]. In both British recommendations, open biopsy is considered for individuals without radiographic focality, and there is stress placed on the need for experienced neurosurgeons and neuropathologists in optimizing tissue procurement and analysis. In all recommendations, the decision to initiate brain biopsy is placed into the context of location and circumstance; whether there are resources available for optimal interpretation, and whether there might be significant changes to clinical actions predicated on the results of tissue analysis, as for example in the distinction of infectious and para-infectious autoimmune disorders. In summary, neuropathology continues to play a vital role in elucidating the nature and pathogenesis of emerging viral infections of the nervous system but has less relevance to the routine management of patients presenting with suspected viral encephalitis and meningoencephalitis. Necrotizing scleritis, conjunctivitis, and other pathologic findings in the left eye and brain of an Ebola virus-infected rhesus macaque (Macaca mulatta) with apparent recovery and a delayed time of death. Zika virus-associated microencephaly: A thorough description of neuropathologic findings in the fetal central nervous system. Frameless robotically targeted sterotactic brain biopsy: Feasibility, diagnostic yield, and safety. Chemokine receptor utilization by human immunodeficiency virus type 1 isolates that replicate in microglia. An insight into recombination with enterovirus species C and nucleotide G-480 reversion from the viewpoint of neurovirulence of vaccine-derived polioviruses. Immune reconstitution inflammatory syndrome of the brain: Case illustrations of a challenging entity. Cytomegalovirus encephalitis in patients with acquired immunodeficiency syndrome: An autopsy study of 30 cases and a review of the literature. The management of encephalitis: Clinical practice guidelines by the infectious diseases society of America. Viral meningoencephalitis: A review of diagnostic methods and guidelines for management. Management of suspected viral encephalitis in children-Association of British Neurologists and British Paediatric Allergy, Immunology and Infection Group national guidelines. Management of suspected viral encephalitis in adults-Association of British neurologists and British Infection Association national guidelines. Consensus guidelines on evaluation and management of suspected acute viral encephalitis in children in India. Case definitions, diagnostic algorithms, and priorities in encephalitis: Consensus statement of the International Encephalitis Consortium. The three neurotropic human herpesviruses vary in the clinical disorders they cause and in their molecular structure. Nevertheless, their genetic material is homologous to a considerable extent, and they share cross-reactivity between their glycoproteins. Likewise, there is a great deal of similarity between the clinical manifestations of the disorders they cause, although they are usually transmitted via different routes and cause primary and recurrent disease in different parts of the body. In recent years, it has been the focus of intensive research aimed at elucidating the molecular basis of its latent nervous system infection and at harnessing this virus as a potential vector for gene therapy. The present review aims at covering all these biological, medical, and neurological aspects of herpes simplex viruses. When clinically apparent, gingivostomatitis and pharyngitis are frequent manifestations, and fever and cervical lymphadenopathy are then common. Following primary infection, an immune response is triggered and seroconversion takes place. Thus, the current prevalence rates may be underestimated, compatible with our own personal experience. This might be attributed mainly to the type of cell that harbors the latent viral genome [15]. These include alterations in consciousness, personality and behavioral disturbances, focal neurological signs, cognitive disturbances, and all types of seizures. Fever is one of the most frequent features at presentation, and its absence should cast doubt upon the diagnosis. Gray matter involvement is a dominant feature: Personality changes, confusion, and disorientation are present in about threefourths of the patients. Occasionally, patients are initially referred for psychiatric consultation because of delusions, agitation, and personality changes. However, definite diagnosis of the causative agent of viral encephalitis is still frustrating, and even under optimal circumstances and with molecular and serological measures, the causative pathogen can be identified in only 50%70% of cases [25]. Meticulous history taking and examination are mandatory to enable correct clinical diagnosis. False-negative results might be present during the first days of the disease, and when in doubt a repeat lumbar puncture after 12 days is indicated. Focal abnormalities (spike and sharp-wave patterns over the involved temporal lobes) or diffuse slowing may be observed. Therefore, if neuroimaging cannot be obtained within the briefest span of time, lumbar puncture should be postponed only when strict contraindications (such as suspicion of increased intracranial pressure due to a lesion of the posterior fossa space) are present. Of note is the observation that the disease can sometimes affect both hemispheres though with different intensity [30] and on rare occasions involve preferentially the brainstem [31]. It contains moderate pleocytosis, usually mononuclear, and red blood cells, reflecting the hemorrhagic nature of the infectious process within brain parenchyma. Serodiagnosis is based on the demonstration of 48 Herpes simplex viruses a relapsing encephalitic illness. When performed, it should be guided by clinical and radiological localization and aimed at obtaining histology and virus isolation that will establish diagnosis beyond doubt. In the last years, it has become increasingly recognized that autoimmune conditions contribute significantly to the spectrum of encephalitis. Clinical suspicion and early diagnosis of autoimmune etiologies are of particular importance due to the need for early institution of effective immunesuppressive therapies. Following cases of relapse after a 10-day course of acyclovir therapy [4749], the current recommended protocols have increased from 10 days of therapy to 2 and even 3 weeks. Because acyclovir has only 15%39% oral absorption, valaciclovir, an acyclovir prodrug for oral administration with better bioavailability, was introduced [5255]. Penciclovir achieves higher intracellular concentrations than acyclovir [56], and famciclovir is a prodrug of penciclovir with better oral bioavailability [57,58]. Additional therapeutic considerations include: Respiratory assistance: this may be used to reduce increased intracranial pressure, and therefore early intubation is generally recommended. Acyclovir is an antiviral compound developed for use against herpes simplex infections on the basis of an idea that was one of the reasons that its inventor, Gertrud B. It is phosphorylated to its active form by the virus-specific thymidine kinase enzyme and prevents viral replication by inhibiting the viral (as well 5. The age of the patient and the level of consciousness at the time of introduction of therapy are prognostic determinants. Cognitive impairment remains the main problem despite early diagnosis and/or treatment and good early outcome [64]. Neonates present with systemic findings (alterations in body temperature, lethargy, respiratory distress, anorexia, vomiting, and cyanosis), and neurological signs (irritability, bulging fontanele, seizures, opisthotonus, and coma) [68]. If not treated immediately, the last pattern will develop into a disseminated condition, which carries the worst prognosis. The skin, eye, and/or mouth findings are present in about 80% of all cases and are highly suggestive of the diagnosis. The condition may resemble bacterial sepsis or meningitis, and therefore laboratory diagnosis is mandatory. This can be done rapidly by isolation of the virus from maternal genital lesions and secretions, by isolation of the virus from the vesicles in the newborn, or by examination of peripheral blood and cerebrospinal specimens from the neonate. Serology cannot be relied upon, because IgG might be maternal and IgM is not produced in the infant until 2 weeks after disease onset.
Discount rulide 150mg buy. Billie Eilish - my strange addiction (Lyrics).
The torque wrench is inserted into the distal port of the ventricular channel of the new pulse generator to be ready to tighten medicine 853 cheap 150mg rulide amex. After disconnecting the black cable medications causing tinnitus rulide 150 mg with amex, an assistant quickly inserts the lead electrode into the header of the pulse generator and the torque wrench is tightened symptoms for hiv purchase rulide 150 mg online. Even if there are two set-screws medications hypothyroidism order online rulide, there is enough contact with the proximal electrode in the header of the pulse generator to enable bipolar pacing after the distal set-screw is tightened treatment of hemorrhoids rulide 150mg buy. Then the proximal set-screw is tightened, and the red cable is no longer required. Placing the atrial lead in the atrial port and tightening those set-screws completes the connections to the pulse generator. Thresholds for sensing likewise tend to increase after lead implantation but less so for steroid-eluting leads. Acceptable measurable intracardiac electrogram amplitudes and slew rates depend on the maximum programmable sensitivity of the new pulse generator. For most systems, P-wave amplitude of 1 mV or more and R-wave amplitude of 3 mV or more constitute minimally acceptable long-term values. Such low amplitudes, however, leave little room for further deterioration in lead function and can lead to problems with sensing. If atrial or ventricular ectopy is present, the operator should determine the electrogram amplitude of ectopic complexes to ensure appropriate sensing by the pacemaker. In patients with paroxysmal atrial fibrillation, excellent atrial sensing may be required to detect atrial fibrillation reliably without signal dropout. Higher-amplitude electrograms are required for chronic unipolar leads to allow programming of lower sensitivities to avoid myopotential sensing. Inadequate sensing or pacing thresholds at the time of generator replacement are indications for placement of a new lead in the affected chamber. The new lead can usually be placed through the same subclavian or axillary vein, although it is preferable to avoid having too many leads (especially more than four) pass through the same vessel, to reduce the chance of venous occlusion and thrombosis. Alternatively, an entirely new generator or lead system may be placed on the contralateral side. If a new system is placed on the contralateral side to avoid vascular overload or due to preexisting occlusion, we prefer to operate on only the new side at the first setting. It is easier to return later to remove an abandoned device that has been inactivated than to risk infection of both operative sites. Examining the Structural Integrity of Leads and the Lead-Generator Interface Visual inspection at surgery provides clues to lead integrity. Fluid inside the lead body suggests an outer insulation break but, especially in coradial pacing leads, does not necessarily mandate lead replacement. Undue tension on the lead near the fixation site may cause kinking, conductor uncoiling, conductor fracture, or thinning of the electric insulator. A hazy appearance of the insulator surrounding an area of tension or repeated stress is common in older leads. This appearance represents surface erosion of the lead insulator and does not itself imply lead malfunction. The finding should, however, alert the operator to the possibility of lead damage in areas of stress to the insulation. An examination of the suture location ensures that the ligature remains around the suture sleeve, and gentle tension on the lead body ensures its fixation at the venous entry site. Visual inspection of the specific course of a coiled lead in the pocket may be hampered by a significant thickness of overlying capsule scar; fluoroscopy can assist in this regard. Direct examination of the lead connector can assist in the identification of the lead model if not previously known. Venography Venography is commonly required as part of the device replacement procedure. Inability to access the subclavian vein that carries a previously implanted lead suggests either an incorrect needle insertion angle or an occluded subclavian or brachiocephalic venous system (Video 34-5). The vein should be approached with the bevel of the needle facing the implanted lead. If access is not possible, venography may provide better delineation of the course of the axillary or subclavian veins. Left upper extremity venography demonstrates complete occlusion of the left subclavian vein around a previously existing transvenous implantable cardioverter-defibrillator lead tunneled to the abdomen. The occlusion occurs at the level of the subclavian vein as it enters the left brachiocephalic vein. Collateral vessels typically branch off at the first point of occlusion and eventually reconstitute at the level that the occlusion ends. If access from the left side is required, extraction of the lead to maintain a conduit would be the only option to pass a new lead to the superior vena cava from this side. Because the pulse generator had reached end of service, lead integrity could not be evaluated noninvasively before the operation to replace the pulse generator. The leads were wrapped around each other 21 times; on unwrapping them, it was clear that both conductors had been fractured. The still photo shows that the continuous manipulation of the device dislodged the atrial lead, the tip of which now is located in the left brachiocephalic vein. The twiddled right ventricular lead coils can be easily seen medial to the pulse generator. Lead extraction was used to remove the failed leads, and two new leads were placed; the new pulse generator was attached to the fascia with nonabsorbable suture to prevent it from being twirled again. If needle placement in the vessel is adequate, failure to pass a wire suggests proximal venous occlusion. Chronic venous occlusion may occur asymptomatically in conjunction with the development of collateral venous circulation around the shoulder. Delineation of the location and length of occlusion indicates to the operator an appropriate needle insertion site for placement of a new lead. Dye is injected directly into the subclavian or axillary vein through the insertion needle, as this local venogram gives the best opacification. Occlusion of the brachiocephalic system proximal to the junction of the internal jugular vein excludes the ipsilateral jugular system as an alternative site for a new lead. Alternatively, if the subclavian vein is occluded and the internal jugular vein remains patent, a new lead may still be placed on the same side using the jugular approach. Finally, leakage of venography dye into perivascular tissues or into the pericardial space suggests vessel or cardiac chamber perforation, respectively. If the patient has had any prior vascular access ipsilateral to the side of the intended new lead implant, we perform venography before incision of the device pocket. Prior vascular access includes subclavian or internal jugular central catheters (both tunneled and nontunneled), tunneled subcutaneous infusion ports, or hemodialysis access ports. The technique is performed by injection of 10 to 20 mL of radiopaque dye (a 50% dilution generally suffices) followed by a brisk saline flush into a vein peripheral to the occlusion site. A, A selection of basic surgical instruments is essential, including hemostats, retractors, anesthetic and needles, sutures, and sponges. These include a variety of sizes of introducers, sheaths and guidewires, and testing cables. Suction is especially important to maintain hemostasis and to flush the pocket, and sterile drapes cover the image intensifier and lights. Most patients require reoperation for elective battery replacement or battery or lead revision, whereas 1% to 6% of patients return to the laboratory for other problems, such as pocket hematoma, pocket twitch, diaphragmatic pacing, and pocket relocation (see Table 34-1). Aspirin and clopidogrel are not stopped before the procedure unless there is a compelling medical reason. The patient fasts from midnight and receives preoperative antibiotics, most commonly being admitted on the day of the procedure. Procedures are routinely performed with local or regional anesthesia, supplemented by intravenous conscious sedation or propofol administered by the anesthesia service. This would be important for patients with significant obstructive sleep apnea syndrome or for those with severely compromised left ventricular systolic function. For conscious sedation, most institutions use a combination of a short-acting, amnestic benzodiazepine such as midazolam together with an intravenous narcotic for analgesia, such as fentanyl. Continuous electrocardiographic monitoring, pulse oximetry, and sterile preparation and draping are standard procedures. These principles are similar to those required at initial implantation (see Box 34-1). To avoid induction of ventricular fibrillation, development of fibrosis at the lead tip, and damage to the generator itself, electrocautery must not be used directly over an implanted pulse generator with unipolar leads. This issue has become much less of a problem with the current exclusive implantation of bipolar leads. Electrocautery can be used safely during battery changes as long as the leads are not grounded to the patient, to avoid current shunting directly to the heart. Hemostasis at reoperation can usually be secured with electrocautery or direct ligature. Use of surgical absorbable cellulose or topical thrombin assists in treating persistently oozy pockets. We find topical coagulants most useful if there is damage to the device capsule and the underlying fascia and muscle tissues have been compromised. Specific Techniques Local anesthesia is administered most commonly as 1% lidocaine (10-20 mL) infiltrated into the scar line from the previous procedure; additional lidocaine may be given under direct vision once the capsule of the pocket has been defined. There is no reason that a new incision line needs to be made with device replacement. Healing will proceed appropriately with approximation of the tissues and a tight surgical closure. The skin and subcutaneous tissues are opened with sharp dissection, which is required to penetrate the tough scar tissue and dermal layer. Deeper dissection with Metzenbaum scissors or electrocautery is carried out to delineate the pacemaker capsule. Once the pocket is reached, the fibrous capsule is sharply incised and then extended under direct visualization of the implanted pulse generator and leads. The capsule must be opened far enough to allow extraction of the pulse generator and lead connector assembly without undue force. The posterior capsule should be carefully dissected away from the leads to allow mobility. Access to leads and generator may be facilitated through the use of self-retaining retractors. Extreme care is required throughout the procedure to preserve the integrity of the leads and lead connectors; they must not be punctured with anesthetic needles or cut with blades or scissors. If electrocautery is used to remove tissue from the leads in dissecting them from scar tissue in the posterior capsule, the probe must keep moving over the lead so as to not overheat the lead insulation and thereby damage it. A, the initial incision to replace the pulse generator has been carried to the capsule surrounding the metallic can, which is clearly visible. The capsule around the device is incised and opened carefully to avoid damage to the leads; occasionally, a lead will be found overlying the generator. Note that the incision is just long enough to fit the device removed and the new device to be placed in the pocket. C, After delivery of the pulse generator, tension on the leads demonstrates that they are heavily fibrosed into the pocket. Electrocautery over the lead insulators proceeds cautiously to avoid insulator damage; the cautery pen must be kept in motion and not linger over any one location on the lead body. Gentle traction is applied to the leads and, when possible, to the scar tissue also. The Plasma blade (Medtronic) may be useful in device replacements to decrease the chance of damage to existing leads. Once the generator is delivered out of the pocket, the leads are disconnected and analyzed. Unipolar pacemaker leads require direct grounding to subcutaneous tissue; the active part of the unipolar generator must remain in contact with the patient before the lead is disconnected. Grounding can best be accomplished through a large surface area ground electrode placed directly into the open pocket. Making contact with this electrode onto the active surface of a unipolar pulse generator allows the generator to be removed safely from the pocket before the lead is disconnected, even in a pacemaker-dependent patient. After being secured to temporary pacing cables, leads can be completely freed of adhesions up to their entry point into the subclavian vein, if necessary, to examine lead integrity or for extraction. We use low-energy electrocautery sparingly to dissect the leads free of adhesions because the scar tissue could be especially tough and adherent to lead structures. If a previously implanted lead is extracted through an occluded vessel using a dilating sheath, a guidewire can usually be inserted into the vascular system through the extraction sheath to maintain a conduit for replacement. In other cases, deep subclavian venipuncture, brachiocephalic cutdown, an internal jugular approach, or tunneling from the other side provide alternative means of inserting a new lead. After the old pulse generator has been detached from leads and lead integrity and functional status have been ascertained, a new pulse generator can be attached. Redundant lead coils are placed posterior to the pulse generator, and the pocket is closed with at least three layers of absorbable suture-two subcutaneous and one subcuticular. The operator should be amenable to place additional layers in patients with a lot of fat tissue to prevent wound dehiscence and to prevent subsequent puckering of the skin over the incision line. At generator replacement or revision, the old capsule needs to be incised or removed. First, a new device, even if an identical model to the one removed, will never fit perfectly in the original pocket without tension, and second, doing so allows for absorption of fluid and fresh blood flow, which are not possible if the relatively avascular capsule is left intact. One can access the subpectoral plane by locating the junction between the sternal and clavicular heads of the pectoralis major muscle and making entry at that point in a bloodless plane, taking care to avoid damage to penetrating neurovascular bundles. Most of these neurovascular bundles are on the posterior aspect of the subpectoral plane.
Anomic Aphasia Anomia (difficulty in finding the correct word) can occur in a variety of conditions treatment receding gums buy rulide 150mg low cost, including toxic and metabolic encephalopathies medicine 369 rulide 150 mg order on-line. When anomia occurs as an aphasic disorder symptoms 4dp5dt fet cheap rulide 150 mg buy, speech may be ftuent but devoid of meaning as a result of word-finding difficulty medications 1 cheap rulide 150mg. The presence of anomic aphasia is oflittle value in localizing the area of dysfunction medications ending in pam order generic rulide pills. Focal lesions throughout the dominant hemisphere or, in some cases, in the nondominant hemisphere, can produce anomic aphasia. Alexia Alexia (the inability to read) can occur as part of aphasic syndromes or as an isolated abnormality. Alexia with Agraphla this disorder, in which there is impairment of reading and writing, is seen with pathologic lesions at the temporal. Top: Horlzontal section with a large high-Intensity area In the temporal lobe, representing an Infarct caused by occlusion of a mlddle cerebral artery branch. Alexia without Agraphia Alexia without agraphia is a striking disorder in which the patient is unable to read. Patients with this disorder are capable of writing a paragraph but, when asked to read it, cannot do so. Written material presented to the left visual field is processed in the visual cortex on the right side. However, neurons in the visual cortex on the two sides are normally interconnected via axons that project through the splenium. As a result of damage to the splenium, visual information in the right visual cortex cannot be transmitted to the visual cortex in the left (dominant) hemisphere and. Conduction Aphasia In this unusual aphasia, verbal output is fluent and paraphasic. Naming is impaired, although the patient often is able to select the correct name from a list. Isolation Aphasias In these unusual aphasias, repetition is spared, but comprehension is impaired. Damage to two regions (the visual cortex In the left, speech-dominant hemisphere and the splenlum of the corpus callosum, which cantes lnterhemlspherlc axons connecting the two visual cortices) Is required. Thus, occluslcn of the left posterior cerebral artefy can produce this stTlklng syndrome. Agnosla Agnosia-difficulty in identification or recognition-is usually considered to be caused by disturbances in the association functions of the cerebral cortex. Astereognosis is a failure of tactile recognition of objects and is usually associated with parietal lesions of the contralateral hemisphere. Visual agnosia, the inability to recognize things by sight (eg, objects, pictures, persons, spatial relationships) can occur with or without hemianopsia on the dominant side. It is a result of parietooccipital lesions or the interruption of fibers in the splenium of the corpus calloswn. Prosopagnolia is a striking syndrome in which the patient loses the ability to recognize familiar faces. Anosognosia, the lack of awareness of disease or denial of illness, may occur together with the unilateral neglect syndrome. Even when may be able to describe identifying features such as eye color, length and color of hair, and presence or absence of a mustache. Although the anatomic basis for this syndrome remains controversial, lesions in the temporal and occipital lobes, in some cases bilateral, have been suggested to be causative. Unilateral negl«t is a syndrome in which the patient fails to respond to stimuli in one half of space, contralateral to a hemispheric lesion. Unilateral neglect is most easily demonstrated following injury to the right cerebral hemisphere (left-sided unilateral neglect). The patient was not aware of his left-sided weakness, and falled to respond to stlmull on his left side. Apraxia Apraxia, the inability to carry out motor acts correctly despite intact motor and sensory pathways, intact comprehension, and full cooperation, can occur following injury to a variety of cortical and subcortical sites. Ideomotor apraxia is the inability to perform motor responses upon verbal command, when these responses were previously carried out spontaneously. For example, the patient may fail to show his teeth on command, although he can do this spontaneously. Providing patients with objects to be used (eg, giving them a hairbrush and asking them to demonstrate how to brush their hair) leads to improvement of their performance. Ideational apraxia is characterized by an abnormality in the conception of movements, so the patient may have difficulty doing anything at all, or may have problems sequencing the different components of a complex act although each separate component can be performed correctly. In ideational apraxia, introduction of objects to be used does not improve performance. Ideational apraxia may be seen after lesions of the left temporalparietal-occipital area. When neurosurgery is contemplated for a patient, it can be useful for one to establish which cerebral hemisphere is dominant for speech. Typically, amobarbital or thiopental sodium is injected into a carotid artery while the patient is counting aloud and making rapidly alternating movements of the fingers of both hands. When the carotid artery of the dominant side is injected, a much greater and longer interference with speech function occurs than with injection of the other side. Immediate recall is the phenomenon that allows people to remember and repeat a small amount of information shortly after reading or hearing it. In tests, most people can repeat, parrot-like, a short series of words or numbers for up to 10 minutes. Tests usually involve short lists of more complicated numbers (eg, telephone numbers) or sentences for a period of an hour or less. The formation of memories appears to involve the strengthening of certain synapses. Experimental and clinical observations suggest that the encoding of long-term memory involves the hippocampus and adjacent cortex in the medial temporal lobes. The presence of this tetrad suggests dysfunction in the angular gyrus of the left hemisphere. The left hemisphere controls language and speech in most people; the right hemisphere leads in interpreting three-dimensional images and spaces. Other distinctions have been postulated, such as music understanding in the left hemisphere, arithmetic and design in the right. Most right-handed people are left-hemisphere dominant; so are 70% ofleft-handed people, while the remaining 30% are righthemisphere dominant. The slope of the left lateral fissure is less steep, and the upper aspect of the left superior temporal gyrus (the planum temporale) is broader in people with left-hemisphere dominance. Epilepsy is characterized by sudden, transient alterations of brain function, usually with motor, sensory, autonomic, or psychic symptoms; it is often accompanied by alterations in consciousness. These are termed focal motor seizures, and they suggest damage to a discrete, specific part of the brain. For example, if the motor cortex for the hand is involved, the seizure may be confined to the hand. Consciousness may be retained, and the seizure may spread over the rest of the adjacent motor cortex to involve adjacent peripheral parts. Electrical stimulation of the exposed cortex during neurosurgery has aided in mapping the cortex and in understanding localized, partial seizures. For example, ele<;trical stimulation of various regions within the primary motor cortex. Thalamus Hippoc:ampus Basal forebrain Brain areas concerned with encoding long-tenn memories. In the broadest sense, they can be categorized into disorders characterized by generallzecl or partial (focal. Some types ofseizures are due to lesions in specific parts of the brain and thus have localizing value. Complex acts and movements such as walking or fastening or unfastening buttons may occur for several seconds or as long as 10 minutes. Temporal lobe foci (spikes, sharp waves, or combinations of these) are frequently associated with this type of epilepsy. This unusual disorder, called antarograda amnesia, Is often seen as a result of bilateral limbic leslons. An example Is provided by herpes sl~ plex encephalltls, which preferentially affects the temporal lobes, and by bilateral posterior cerebral Infarcts, which may damage both temporal lobes. Lesions of the medial thalamus (partlcularly the dorsomedlal nuclel) can also cause anterograde amnesia; this can occur as a result of tumor and Infarctions. Memory deficit Is also common In the Wemlcka-Korsakoff syndrome, In which hemorrhaglc lesions develop In the medial thalamlc nude! In all of the above disorders, retrograde amnesia, that Is, the loss of memory for events prTor to the lesion, can also occur. Her seizures were characterized by an aura consisting of a rising sensation In her gut. Her seizures averaged 5 to 10 per month despite treatment with antlconvulsant drugs. Because of the failure of traditional medlcal therapy to control her seizures, the patient was hospltallzed. Elect~ encephalogram monitoring revealed slowlng and abnormal spike activity In the right anterior temporal lobe. In which an anesthetlc was Injected Into her carotid arteries, demonstrated left-hemisphere dominance for speech and a marked disparity of memory function between the left and right hemispheres; the left hemisphere showed perfect memory and the right showed slgnlficantly Impaired memory. Subsequent to surgery, the patient has had no seizures with the exception of one that occurred when her antlconvulsant drug levels were very low. This case Illustrates a classical history and findings for the most common form of epilepsy treated by surgery, medlal temporal lobe epilepsy. The correlation of anatomic localization by electrlcal, structural, and cognitive studies preoperatlvely and the subsequent response to resection of a circumscribed cerebral area provide a dramatic demonstration of anatomlc-cllnlcal correlation. The patiem was slow to respond but roughly oriented with regard to person, place, and time. The pupils responded to light and there One month before admission, this was slight. Other findings included decreased appreciation of pain on the left side of the face, complete paralysis ofthe left central face, and complete flaccid paralysis of the left arm and less severe weakness of the left leg; the patient seemed to ignore the left side of her body and was not concerned about her hemiparesis. Physical examination revealed cataracts in both eyes, which were not severe enough to compromise vision signilicantly. A 63-year~d clerk suddenly experienced a strange feeling over bis body, which he characterized as an electric shock, with flashes of blue light on the right During this episode he felt confused. He did not notice bis wife bringing him a cup of coffee as she approached from bis right side. During the next 2 weeks, he continued to bump into objects on bis right side and complained of poor vision, which he atttibuted to a cataract in his right eye. Angiography can also be used to determine whether the position of the vessels in relation to intrac:ranial structures is normal or pathologically changed. Right and left internal carotid and vertebral angiognms may be complemented by other films (eg, by an external carotid series in cases of meningioma or arteriovenous malformation). The films are often presented as the brain and its vessels, and spaces in the brain containing cerebrospinal fluid can aid immeasurably in the localization of lesions. In concert with physical examination and history, imaging studies can provide important clues to diagnosis. In emergency cases, images of unconscious patients may be the only diagnostic: information available. It is essential for the clinician to understand the various imaging modalities that are available and to order the most useful tests. It is also essential to correlate results of imaging with the clinic:al picture, that is, with the history and neurologic:al examination. Plain films of the skull can define the extent of a skull fracture and a possible depression or determine the presence ofcalcified brain lesions, foreign bodies, or tumors involving the skull. They can provide images of the bony structures and foramens at the base of the skull and of the sinuses. Skull x-ray films can also provide evidence for c:hronic:ally increased intracranial pressure, accompanied by thinning of the dorsum sellae, and abnormalities in the size and shape of sella turc:ic:a, which suggest large pituitary twnors. It bas become a primary tool for demonstrating the presence ofabnor- mal calcifications. Correlation with the clinical history and physical examination is an absolute requirement. Black-and-white pictures of head slices are then displayed, with black representing low-density structures and white representing high-density structures. Detailed examination of orbital contents requires planes at right angles to the orbital axis. It depicts protons and neutrons in a strong external magnetic field shielded from extraneous radio signals; no radiation is used. Images reformed by a computer from a series of thin sections allow visualization in any des. Line 1 Is at the level of the fora men magnum; line 4 ls at the level of the lnfraorbltomeatal plane. Dilated ventricles in a 7-year-old boy who had undergone a shunting operation at age 1 year. A: Image obtained with a short time sequence: the gray-whlte boundaries are poorly defined, and the spaces filled with cerebrosplnal fluid are dark. C: Image obtained with a long time sequence; the white matter is clearty differentiated from gray matter, and the spaces filled with cerebrosplnal fluid are white.
References
- Muellejans B, Matthey T, Scholpp J, Schill M. Sedation in the intensive care unit with remifentanil/propofol versus midazolam/fentanyl: a randomised, open-label, pharmacoeconomic trial. Crit Care. 2006;10:R91.
- Wagenvoort CA, Nauta J, van der Schaar PJ, Weeda HW, Wagenvoort N. Vascular changes in pulmonic stenosis and tetralogy of Fallot studied in lung biopsies. Circulation 1967;36(6):924-32.
- Armstrong AB, Wang M, Eble JN, et al: TP53 mutational analysis supports monoclonal origin of biphasic sarcomatoid urothelial carcinoma (carcinosarcoma) of the urinary bladder, Mod Pathol 22:113n118, 2009.
- Kissane DW, Love A, Hatton A, et al. Effect of cognitive-existential group therapy on survival in early-stage breast cancer. J Clin Oncol 2004;22(21):4255-4260.
- Haans LC, Laven JS, Mali WP, et al: Testis volumes, semen quality, and hormonal patterns in adolescents with and without a varicocele, Fertil Steril 56:731n736, 1991.
- Stojkovic T, Latour P, Viet G, et al. Vocal cord and diaphragm paralysis, as clinical features of a French family with autosomal recessive Charcot-Marie-Tooth disease, associated with a new mutation in the GDAP1 gene. Neuromuscul Disord. 2004;14(4):261-264.