
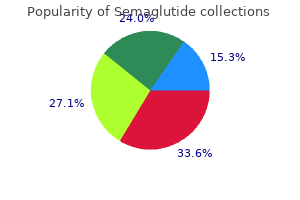
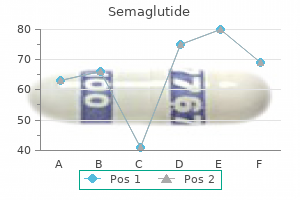
Semaglutide
| Contato
Página Inicial
Enzo J. Sella, MD
- Associate Clinical Professor of Orthopaedics and Rehabilitation
- Yale University School of Medicine
- Co-Director of Foot and Ankle Clinics
- Yale New Haven Hospital
- Section Chief of Orthopaedics
- St Raphael Hospital
- New Haven, Connecticut
It is not unheard of for the laboratory to receive a blood glucose request on a specimen taken from the same arm into which 5% glucose is being infused weight loss pills that are fda approved semaglutide 14 mg mastercard. Usually the results are biochemically incredible but it is just possible that they may be acted upon with disastrous consequences for the patient weight loss in dogs purchase genuine semaglutide. A blood sample stored overnight before being sent to the laboratory will show falsely high potassium weight loss 05 kg per week order 14 mg semaglutide with visa, phosphate and red cell enzymes weight loss pills similar to adipex generic semaglutide 14 mg with visa, such as lactate dehydrogenase weight loss pills energy cheap semaglutide 14 mg on line, because of leakage into the extracellular fluid from the cells. How often depends on how quickly significant changes are liable to occur, and there is little point in requesting repeat tests if a numerical change will not have an influence on treatment. The main reason for asking for an analysis to be performed on an urgent basis is that immediate treatment depends on the result. Specimens may be required for haematology, microbiology, virology, immunology and histopathology, and all require similar attention to detail in filling out request forms and obtaining the appropriate samples for analysis. Case history 1 A blood specimen was taken from a 65-year-old women to check her serum potassium concentration as she had been on thiazide diuretics for some time. The use of the laboratory n Each biochemistry test request should be thought of as a question about the patient; each biochemical result as an answer. Request forms and specimens must be correctly labelled to ensure that results can be communicated quickly to the clinician. Many biochemical tests are performed on serum, the supernatant obtained from centrifugation of clotted blood collected into a plain container. Others require plasma, the supernatant obtained when blood is prevented from clotting by an anticoagulant. Changes in concentration can occur for two reasons: n Precision and accuracy Precision is the reproducibility of an analytical method. It is the objective in every biochemical method to provide good precision and accuracy. How biochemical results are expressed Most biochemical analyses are quantitative, although simple qualitative or semiquantitative tests, such as those for the presence of glucose in urine, are commonly encountered methods used for point of care testing. Many tests measure the amount of the analyte in a small volume of blood, plasma, serum, urine or some other fluid or tissue. Results are reported as concentrations, usually in terms of the number of moles in one litre (mol/L) (Table 3. Enzyme assays are carried out in such a way that the activity measured is directly proportional to the amount of enzyme present. Large molecules such as proteins are reported in mass units (grams or milligrams) per litre. Analytical sensitivity and specificity the analytical sensitivity of an assay is a measure of how little of the analyte the method can detect. Analytical specificity of an assay relates to how good the assay is at discriminating between the requested analyte and potentially interfering substances. The expected values are known and the actual results obtained are compared with previous values to monitor performance. In external quality assurance programmes, identical samples are distributed to laboratories; results are then compared. These include: n n (b) n n precision and accuracy sensitivity and specificity quality assurance reference intervals. Concentration is always dependent on two factors: the amount of solute and the amount of solvent. The concentration of the sugar solution in the beaker can be increased from 1 spoon/ beaker (a) to 2 spoons/beaker by either decreasing the volume of solvent (b) or increasing the amount of solute (c). Sensitivity is a measure of the incidence of positive results in patients who are known to have a condition. As noted above, the use of the terms specificity and sensitivity in this context should not be confused with the same terms used to describe analytical performance. An ideal diagnostic test would be 100% sensitive, showing positive results in all diseased subjects, and 100% specific, with negative results in all persons free of the disease. Reference interval False Other factors When the numbers have been generated, they still have to be interpreted in the light of a host of variables. The clinician can refer to the patient or to the clinical notes, whereas the biochemist has only the information on the request form to consult. The clinician may well ask the following questions on receiving a biochemistry report: n (a) positives Number of tests High specificity Low sensitivity Diagnostic cut-off Test value (b) Number of tests Biological factors affecting the interpretation of results the discrimination between normal and abnormal results is affected by various physiological factors that must be considered when interpreting any given result. This means that, by definition, 5% of any population will have a result outside the reference interval. In practice there are no rigid limits demarcating the diseased population from the healthy; however, the further a result is from the limits of the reference interval, the more likely it is to indicate pathology. Reference intervals for some analytes such as serum creatinine are different for men and women. There may be different reference intervals for neonates, children, adults and the elderly. The sample may be inappropriate if taken when the patient is fasting or after a meal. Infection and/or tissue injury can affect biochemical values independently of the disease process being investigated. The rest of this book deals with the biochemical investigation of patients and the interpretation of the results obtained. Clinical note It is important to realize that an abnormal result does not always indicate that a disease is present, nor a normal result that it is not. Beware of over-reacting to the slightly abnormal result in the otherwise healthy individual. The interpretation of results n Biochemistry results are often reported as concentrations. Concentrations change if the amount of the analyte changes or if the volume of solvent changes. Variability of results is caused by both analytical factors and biological factors. Different reference intervals may apply depending on the age or sex of the patient. Sequential changes observed in cumulative reports when placed in clinical context are as important as the absolute value of the result. If a result does not accord with that expected for the patient, the finding should be discussed with the laboratory reporting office and a repeat test arranged. Convenience and the desire to know results quickly, as well as expectation of commercial profit by the manufacturers of the tests, have been the major stimuli for these developments. However, it is important to ensure that the limitations of any test and the significance of the results are appreciated by the tester to avoid inappropriate intervention or unnecessary anxiety. Many are conveniently measured, semi-quantitatively, using test strips which are dipped briefly into a fresh urine sample. Any excess urine is removed, and the result assessed after a specified time by comparing a colour change with a code on the side of the test strip container. The information obtained from such tests is of variable value to the tester, whether patient or clinician. The tests commonly performed away from the laboratory can be categorized as follows: A. They clearly give valuable information and allow the practitioner to reassure the patient or family or initiate further investigations or treatment. In the Accident and Emergency setting, extreme caution must be taken before one can fully ascribe confusion in a patient with head injury to the effects of alcohol, a common complicating feature in such patients. The most common blood test outside the laboratory is the determination of glucose concentration, in a finger stab sample, at home or in the clinic. Diabetic patients who need to monitor their blood glucose on a regular basis can do so at home or at work using one of many commercially available pocket-sized instruments. These analysers may be used Methodology It is a feature of many sideroom tests that their simplicity disguises the use of sophisticated methodology. The test is simple to carry out; a few drops of urine are placed in the sample window, and the result is shown within 5 minutes. A third antibody recognizes the constant region of the first antibody and binds the excess, thus providing a control to show that sufficient urine had been added to the test strip, the most likely form of error. Many of these tests are expensive alternatives to the traditional methods used in the laboratory. This additional expense must be justified, for example, on the basis of convenience or speed of obtaining the result. The person performing the assay outside the laboratory (the operator) must assume a number of responsibilities that would normally be those of the laboratory staff. There is the responsibility to perform the assay appropriately and to provide an answer that is accurate, precise and meaningful. Tests designed for use outside the laboratory are robust but are by no means foolproof. Most operators will not be trained laboratory technicians but patients, nurses or clinicians. If an assay is performed in an individual of inappropriate age, sex, or at the wrong time of day, or month, then the result may be clinically meaningless. Similarly, the nature of the sample collected for analysis should be considered when interpreting the result. Where the results seem at odds with the clinical situation, interference from contaminants. The future There is no doubt that in the future, biochemical testing of patients at the point of care will become practical for many of the analytes currently measured in the laboratory. There is, however, likely to be much debate about costs and the clinical usefulness of such nonlaboratory-based analyses. Case history 2 At a village fete, a local charity group was fundraising by performing certain sideroom tests. His family was concerned, and an hour later his cousin, a recently diagnosed diabetic, confirmed the hyperglycaemia with his home monitoring equipment, and found glycosuria +++. All of these problems can be readily overcome by following instructions carefully. Regular maintenance of the equipment may be necessary, and simple quality control checks should be performed. It should always be possible to arrange simple quality control cross checks with the main biochemistry laboratory. Interpretive problems Even when analytically correct results are obtained, there are other problems 6 Positive result Point of care testing Negative result n Many biochemical tests are performed outside the normal laboratory setting, for the convenience of patient and clinician. Although apparently simple, such tests may yield erroneous results because of operator errors. It is important that advice be readily available to interpret each result in the clinical context. In the absence of this approach, individual laboratories should use reference intervals that are based on values obtained from subjects appropriately selected from local populations, but this is not always feasible. The list is not intended to be comprehensive; it is merely provided for guidance in answering the cases and examples in this book. Please note that age- and/or sex-specific reference intervals are available for a range of analytes including alkaline phosphatase, creatinine, and urate. Glucose, insulin and triglyceride all rise postprandially and should, where possible, be measured in the fasting state. The inlet supply represents fluids taken orally or by intravenous infusion, while the outlet is normally the urinary tract. Selective loss of fluid from each of these compartments gives rise to distinct signs and symptoms. Intracellular fluid loss, for example, causes cellular dysfunction, which is most notably evident as lethargy, confusion and coma. The water tank model illustrates the relative volumes of each of these compartments and can be used to help visualize some of the clinical disorders of fluid and electrolyte balance. It is important to realize that the assessment of the volume of body fluid compartments is not the undertaking of the biochemistry laboratory. Inlet Normal Extracellular fluid compartment Intracellular fluid compartment Normal Outlet (a) Water tank model of body fluid compartments. Clinical assessments of skin turgor, eyeball tension and the mucous membranes are not always reliable. Ageing affects skin elasticity and the oral mucous membranes may appear dry in patients breathing through their mouths. Electrolytes Sodium (Na+) is the principal extracellular cation, and potassium (K+), the principal intracellular cation. Clinically, the simplest is: Serum osmolality = 2 × serum [sodium] [mmol/kg] [mmol/L] this simple formula only holds if the serum concentration of urea and glucose are within the reference intervals. If either or both are abnormally high, the concentration of either or both (in mmol/L) must be added in to give the calculated osmolality. Sometimes there is an apparent difference between the measured and calculated osmolality. This is achieved by the movement of water across semipermeable membranes in response to concentration changes. Sodium ions are present at the highest concentration and hence make the largest contribution to the total plasma osmolality (see later). Urea and creatinine concentrations provide an indication of renal function, with increased concentrations indicating a decreased glomerular filtration rate (see pp. Concentration Remember that a concentration is a ratio of two variables: the amount of solute. For example, a sodium concentration of 140 mmol/L may become 130 mmol/L because the amount of sodium in the solution has fallen or because the amount of water has increased (see p. Body compartments are separated by semipermeable membranes through which water moves freely. The osmolality of a solution is expressed in mmol solute per kilogram of solvent, which is usually water.
After repeated transvaginal ultrasonography weight loss pills that celebrities use semaglutide 14mg buy with amex, because of abnormal findings of color flow Doppler imaging weight loss xyngular semaglutide 14 mg buy amex, 19 patients underwent surgery weight loss pills heart palpitations semaglutide 14 mg purchase amex. Bell and colleagues reviewed 25 studies on screening for ovarian cancer weight loss pills all natural generic semaglutide 14mg fast delivery, 16 studies on women at average risk weight loss games cheap semaglutide 14mg with amex, and 9 studies on women at higher risk. Many of the studies were small and imprecise on methodology; few gave follow-up details. Some studies used single screening techniques, whereas others used multimodal screening. For women at average risk, 75% of primary cancers were stage I when they were detected with ultrasonography and 50% were stage I when they were detected by multimodal screening (see Table 11-9). In women at higher risk, 60% of tumors detected by screening were stage I; but most important, if low malignant potential tumors were excluded, only 25% were stage I. Falsenegative rates were higher in the higher risk population than in the group at average risk. The false-negative data, when applied to a population with an annual incidence of 40 per 100,000, imply that 30 to 60 surgical procedures would be carried out for every cancer detected at annual gray-scale ultrasonography (assuming 100% sensitivity), and 2. Even if screening detects all ovarian cancers and these are treated with 100% success, the absolute reduction in mortality would be only 1 in about 2500 screened women per year. This is much smaller than the complication rate from unnecessary diagnostic surgery or recall for further tests. Currently, however, there are no reliable data that screening for ovarian cancer is effective in improving length and quality of life in women with ovarian cancer. Yurkovetsky and colleagues reported the results of their screening panel of four biomarkers, with 86% sensitivity at 98% specificity for detecting early-stage disease, and additional studies looking at additional biomarkers are ongoing. These techniques may also offer useful guidelines for predicting therapeutic response and for treatment selection. Currently available technology for screening should be used in the context of clinical trials to determine the efficacy of these modalities and their effect on ovarian cancer mortality. In addition, research must be continued to identify additional markers and imaging techniques that will be useful. Although these same recommendations still hold, we may have better techniques for screening as the data from ongoing trials mature. If a woman has one first-degree relative with ovarian cancer (making her lifetime risk of developing the disease 5%) but no clinical trials are available to her, she may feel that despite the absence of prospective data, this is sufficient risk for her to be screened. This opportunity for screening should be available to the woman and her physician. If a woman were undergoing pelvic surgery, removal of the ovaries at that time would almost fully eliminate her risk of ovarian cancer (although there remains a small risk of peritoneal cancer). If the woman is premenopausal, discussion of estrogen replacement therapy is important before removal of the ovaries because for some younger women, if estrogen replacement is not used, the risk of premature menopause and the potential for osteoporosis may outweigh the risk of ovarian conservation and the potential for ovarian cancer. However, pelvic examination remains the most practical means of detecting early disease. Pain is usually a late complication; it is seen with early disease only in association with a complication such as torsion; rupture; or, rarely, infection. The physician should have a high index of suspicion for an early ovarian neoplasm in any ovary palpated in a patient 3 years or longer after menopause. These patients should be considered for immediate laparoscopy or laparotomy when ultrasound examination findings suggest malignant change. Routine laboratory tests are not of great value in the diagnosis of ovarian tumors. Pelvic ultrasound examination or abdominal radiography may reveal calcifications consistent with myomas or toothlike calcifications consistent with benign teratomas. Intravenous pyelography may be helpful in ruling out disease in adjacent pelvic structures. A barium enema study should be considered in a woman with lower intestinal symptoms. A similar comment can be made for colonoscopy and upper gastrointestinal endoscopy in patients who have lower or upper intestinal symptoms, respectively. Paracentesis for the purpose of obtaining a cell block and cytologic smear of the peritoneal fluid appears unnecessary and is not indicated. If one is dealing with a self-contained malignant cyst, such a procedure can result in spillage of malignant cells into the peritoneal cavity. Regardless of whether the fluid contains neoplastic cells, laparotomy is still necessary to remove the large benign neoplasm or to define the extent of the malignant process. In addition, up to 50% of ascitic fluid samples from patients with true ovarian malignant neoplasms will be negative for malignant cells on cell block analysis. A Pfannenstiel incision is ill-advised in a patient suspected of having an ovarian malignancy. Although lymphatic spread to retroperitoneal nodes is common in ovarian cancer, the disease most often spreads intraperitoneally; free-floating cells shed from the primary tumor are capable of implanting on any peritoneal surface. Any peritoneal fluid (ascites) found when the peritoneal cavity is opened should be aspirated and submitted for cytologic examination. These specimens are obtained by lavaging these areas with 50 to 75 mL of saline solution and retrieving the fluid for cell block analysis. Care should be taken to visualize and palpate all peritoneal surfaces, particularly the underside of the diaphragm, the surface of the liver, the lateral abdominal gutters, and the small and large bowel mesentery. Fiberoptic light sources are particularly helpful in properly visualizing the peritoneal surfaces of the upper abdomen through a vertical lower abdominal incision. The omentum should be removed because microscopic disease is often present in the omentum that is not obvious grossly. If the disease is limited to the pelvis, great care should be taken to avoid rupture of the neoplasm during its 11. Positive ascites or peritoneal washing C One or both ovaries with capsule ruptured or tumor on ovarian surface; malignant cells in ascites or peritoneal washings. E Extension and/or implants to other pelvic tissues; pelvic wall, broad ligament, adjacent peritoneum, mesovarium. G Tumor on liver capsule Pleural fluid (positive cytology) Lung parenchymal metastases Omental cake Lymph node metastases H Peritoneal metastasis beyond pelvis 2 cm in greatest dimension and/or regional lymph node metastasis. All roughened or suspicious surfaces in the peritoneal cavity should be removed as biopsy specimens. This includes adhesions, which should be excised, not incised, because they often contain microscopic disease. Several studies are under way to investigate the efficacy of "blind" peritoneal biopsies and routine retroperitoneal node dissections in the proper staging of early epithelial cancer of the ovary (Table 11-12). Any abnormal-appearing surface is always regarded as suspicious, and biopsies are readily performed. Proper staging is important for treatment planning and for providing an accurate prognosis (Table 11-13). They have also been called proliferative cystadenomas and tumors of low malignant potential and are more completely discussed in Chapter 10. Histologic appearance with prominent fibrous stalks and nonmucinproducing epithelial cells. Although symptomatic recurrence and death may rarely develop as late as 20 years after therapy, these neoplasms are correctly labeled as being of low malignant potential. Most gynecologic oncologists recommend conservative therapy, especially in patients who are desirous of further childbearing and have stage Ia disease (see Chapter 10). Most large studies demonstrate that these different histologic types have similar outcomes with existing therapy, stage for stage and grade for grade. There are ongoing studies to investigate targeted therapies in certain cell types, most notably mucinous and clear cell cancers. Based on our current data, however, prognosis, survival, and therapy for these various forms of epithelial cancer will be considered collectively. The unifocal theory of ovarian epithelial cancer growth suggests that the disease initially grows locally, invading the capsule and mesovarium, and then invades adjacent organs by local extension and lymphatic spread. When the malignant neoplasm reaches the external surface of the capsule, cells exfoliate into the peritoneal cavity, where they circulate and implant on free peritoneal surfaces. Spread to the aortic lymph nodes through lymphatics in the infundibulopelvic ligament is also common. Woodruff suggested a multifocal mechanism of disease spread, whereby the entire coelomic epithelium can give rise to this lesion after exposure to carcinogenic agents that enter the peritoneal cavity from the vagina through the fallopian tubes. Indeed, the lesion could then originate in a multifocal distribution, "like a measles rash," over large portions of the coelomic epithelium. Although the early precursors leading to advanced ovarian cancer are incompletely understood, more current molecular evidence favors the unifocal origin theory. Regardless of origin, the most important prognostic variable for each patient is the extent, or "stage," of disease. A staging system has been devised that allows treatment results in patients with similar prognostic factors to be compared between different institutions. Survival is affected by the cancer stage, the grade of differentiation, the gross findings at surgery (Table 11-14), the amount of residual tumor after surgery, and the additional treatment required. Stages Ia, Ib, and Ic Careful surgical staging is critical in the management of stage I invasive ovarian cancer and should include bilateral salpingo-oophorectomy, hysterectomy, omentectomy, and pelvic and aortic lymph node sampling, with 302 11. Accurate staging forms the cornerstone of clinical decision-making regarding the type and duration of adjuvant therapy. Pelvic and aortic lymph nodes may be involved 10% to 20% of the time in apparent stage I disease, and lymphadenectomy is an important diagnostic and therapeutic procedure. Baiocchi and associates reviewed their experience in 242 women who had pelvic and aortic lymphadenectomy in whom cancer was apparently confined to the ovaries (stage I), and nodal metastasis was found in 32 patients (13%). Patients with serous adenocarcinoma had the highest incidence of node metastasis (25%). There were 33 women with low malignant potential tumors, and 7 (21%) had nodal metastasis. When only one to three nodes were involved, metastases were usually ipsilateral, but these patients could also have metastases to the common iliac or aortic nodes. Accumulated reports of lymph node metastases in clinical stage I ovarian cancer patients are shown in Table 11-15. Without thorough surgical staging, occult metastasis may be present and missed, leading to inadequate subsequent therapy. The use of adjuvant therapy and its role in stage I ovarian cancer continues to be investigated. The 5-year survival in both arms of the study was excellent (>90%) and did not justify the additional toxicity and risks associated with melphalan in this patient population. These patients were randomly assigned to receive melphalan or intraperitoneal colloidal 32P. Survival and disease-free survival were similar in both arms of the study (approximately 80%), and the frequency of severe side effects was low in both arms. Survival was slightly better in the combination chemotherapy arm, and although not statistically significant, the lower rate of complications and side effects in the chemotherapy arm led to the conclusion that platinum-based chemotherapy was preferred. European investigators have also reported their experience with platinum-based therapy in early-stage ovarian cancer. More than 900 patients with early-stage ovarian cancer received either platinum-based adjuvant chemotherapy or observation until chemotherapy was indicated. After a median follow-up of more than 4 years, the improved overall survival (82% chemotherapy vs 74% observation) and recurrence-free survival (76% vs 65%, respectively) at 5 years favored treatment with platinum-based therapy. Although not all patients had undergone comprehensive staging, a subgroup analysis of these patients was reported. Over a 3-year interval, 457 patients were enrolled and evaluated after a median follow-up of 6. The results of the trial have been reported, and although the recurrence rate was 20% lower in patients receiving extended paclitaxel, the result was not statistically significant and there was no appreciable difference in overall survival. In the young woman with stage Ia disease who is desirous of further childbearing, unilateral salpingooophorectomy may be associated with minimal increased risk of recurrence, provided a careful staging procedure is performed and due consideration is given to grade and apparent self-containment of the neoplasm. After conservative treatment for invasive ovarian cancer, term delivery rates have been reported as high as 30%, and successful pregnancy outcomes have been reported after adjuvant chemotherapy. A careful discussion regarding the risks and benefits of this approach is essential because Maltaris and colleagues reported that 12% of patients undergoing fertility-sparing ovarian cancer surgery experienced recurrence and 4% of patients died from their disease. In the management of stage I ovarian cancer the physician must weigh the possible benefits of adjuvant chemotherapy against the risks. We favor treatment with platinumbased combination chemotherapy despite the fact that no clear data show a survival advantage over singleagent therapy. Although historically the role of pelvic and abdominal irradiation and intraperitoneal 32P has been described, the radioisotope and irradiation treatment approaches have all but faded from frontline therapy for ovarian carcinoma. In addition, every reasonable effort should be made to remove all visible ovarian tumors. Most centers prefer combination platinum-based chemotherapy, usually carboplatin and paclitaxel, for this group of patients because of the excellent response rates reported in the literature (see later section on combination chemotherapy and intraperitoneal therapy). If after primary chemotherapy the patient has no clinical evidence of disease (clinical complete response), a second-look procedure was often considered in the past to ascertain the presence of subclinical residual 304 11. The role and benefit of surgical cytoreduction in these patients is detailed in the next section. In the 1970s Griffiths and coworkers evaluated the importance of postsurgical tumor residual by using a multiple linear regression equation with survival as the dependent variable to control simultaneously for the multiple therapeutic and biologic factors that contribute to the ultimate outcome in the individual patient. The most important factors proved to be histologic grade of the tumor and size of the largest residual mass after primary surgery. The operation itself contributed nothing to survival unless it effected reduction in the size of the largest residual tumor mass below the limit of 1. Cytoreductive or "debulking" procedures have gained considerable attention in the management of ovarian cancer. The concept is to reduce the residual tumor burden to a level that subsequent chemotherapy can be most effective.
Serum osmolality = 310 mmol/kg Urine osmolality = 110 mmol/kg Urine volume = 8 litres/24 h Is a water deprivation test required to make the diagnosis in this patient Investigation of renal function (2) n Specific tests are available to measure urinary concentrating ability and ability to excrete and acid load weight loss lunch order cheapest semaglutide and semaglutide. A comparison of urine and serum osmolality measurements will indicate if a patient has the ability to concentrate urine weight loss pills mens health generic 14 mg semaglutide otc. Chemical analysis of renal stones is important in the investigation of their aetiology weight loss quotes tumblr semaglutide 14mg online. Urinalysis comprises a range of analyses that are usually performed at the point of care rather than in a central laboratory weight loss challenge discount semaglutide 14mg buy on line. The strip is held close to the colour blocks on the chart and matched carefully slim9 weight loss pills buy generic semaglutide online, and then discarded. The range of components routinely tested for in commonly available commercial urinalysis strips is extensive and includes glucose, bilirubin, ketones, specific gravity, blood, pH (hydrogen ion concentration), protein, urobilinogen, nitrite and leucocytes (white blood cells). Urinalysis is one of the commonest biochemical tests performed outside the laboratory. Although the test is simple, failure to follow the correct procedure may lead to inaccurate results. A frequent example of this is where test strips are read too quickly or left too long. Other potential errors may arise because test strips have been stored wrongly or are out of date. Glucose the presence of glucose in urine (glycosuria) indicates that the filtered load of glucose exceeds the ability of the renal tubules to reabsorb all of it. This usually reflects hyperglycaemia and should, therefore, prompt consideration of whether more formal testing for diabetes mellitus is appropriate. The renal threshold for glucose may be lowered, for example in pregnancy, and glucose may enter the filtrate even at normal plasma concentrations (renal glycosuria). Blood glucose rises rapidly after a meal, overcoming the normal renal threshold temporarily (alimentary glycosuria). Only the conjugated form is watersoluble, so bilirubinuria signifies the presence in urine of conjugated bilirubin. Conjugated bilirubin is normally excreted through the biliary tree into the gut where it is broken down; a small amount is reabsorbed into the portal circulation, taken up by the liver and re-excreted in bile. Interruption of this so-called enterohepatic circulation usually stems from mechanical obstruction, and results in high levels of conjugated bilirubin in the systemic circulation, some of which spills over into the urine. The renal tubules normally excrete hydrogen ions by mechanisms that ensure tight regulation of the blood hydrogen ion concentration. Dipstick tests for blood are able to detect haemoglobin and myoglobin in addition to red blood cells the presence in the urine sediment of large numbers of red cells establishes the diagnosis of haematuria. The absence of red cells, despite a strongly positive dipstick test for blood, points towards myoglobinuria or haemoglobinuria. Nitrite this dipstick test depends on the conversion of nitrate (from the diet) to nitrite by the action in the urine of bacteria that contain the necessary reductase. Urobilinogen In the gut, conjugated bilirubin is broken down by bacteria to products known collectively as faecal urobilinogen, or stercobilinogen. However, unlike bilirubin, urobilinogen is found in the systemic circulation and is often detectable in the urine of normal subjects. Thus the finding of urobilinogen in urine is of less diagnostic significance than bilirubin. Leucocytes the presence of leucocytes in the urine suggests acute inflammation and the presence of a urinary tract infection. For this reason it is important to check that the dipstick test is not also positive for blood or leucocytes (white cells); it may also be appropriate to screen for a urinary tract infection by sending urine for culture. These samples should be collected into sterile containers and sent to the laboratory without delay for culture and antibiotic sensitivity tests. Their presence usually indicates that the body is using fat to provide energy rather than storing it for later use. This can occur in uncontrolled diabetes, where glucose is unable to enter cells (diabetic ketoacidosis), in alcoholism (alcoholic ketoacidosis), or in association with prolonged fasting or vomiting. Blood the presence of blood in the urine (haematuria) is consistent with various Case history 11 A patient attending an obesity clinic is found to have ketonuria on urinalysis. There is no glycosuria and point-of-care glucose measurement using a strip test is 5. Specific gravity this is a semi-quantitative measure of urinary density, which in turn reflects concentration. Assessment of urinary specific gravity usually just confirms the impression gained by visually inspecting the colour of the urine. When urine concentration needs to be quantitated, most people will request urine osmolality, which has a much wider working range. Chemical analysis of a urine specimen is carried out using commercially available disposable strips. The range of components routinely tested for includes glucose, bilirubin, ketones, specific gravity, blood, pH, protein, urobilinogen, nitrite and leucocytes. It is associated with renal and cardiovascular disease; it identifies diabetic patients at risk of nephropathy and other microvascular complications; and it predicts endorgan damage in hypertensive patients. Although proteinuria may arise through various mechanisms (see below), it is most often an indication of abnormal glomerular function. This is known as the nephrotic syndrome (defined in terms of protein excretion more than 3 g daily). This condition involves malignant proliferation of a clone of plasma cells (a special kind of lymphocyte, the function of which is to produce immunoglobulins). This results in the production of vast amounts of the immunoglobulin produced by the malignant clone. Bence-Jones proteins are light chain fragments of the immunoglobulin that can be detected in the urine. Tubular proteinuria Some proteins are so small that, unlike albumin and other larger proteins, they pass through the glomerulus freely. If these proteins are detected in excess in the urine, this reflects tubular rather than glomerular dysfunction, i. However, tubular function is normally investigated in other ways, and the measurement of these proteins in urine is normally confined to the screening and detection of chronic asymptomatic tubular dysfunction, or a small number of specific clinical scenarios. TammHorsfall proteinuria this glycoprotein gets its name from the authors of a 1952 paper describing its purification. Its significance lies in the fact that, unlike the other proteins mentioned above, it is not derived from the blood, but rather is produced and secreted into the filtrate by the thick ascending limb of the loop of Henle. It forms large aggregates that, when concentrated, can in turn form urinary casts (gel-like cylindrical structures that reflect the shape of the renal tubules and that get dislodged and pass into the urine). When Overflow proteinuria Overflow proteinuria occurs when the ability of the glomeruli to hold back Normal Overflow Glomerular Tubular Secreted. Dipsticks are commercially available disposable strips, impregnated with coloured reagent blocks, which are immersed in urine. The reagents in each block react with a specific component of urine in such a way that the block changes colour if the component is present. Protein is just one of several components tested for; others include glucose, blood and bilirubin. It is convenient for both patient and clinician, and provides a near-instant result at the point of care. However, it gives only a rough indication of the presence or absence of pathological proteinuria, and cannot be used alone to diagnose or exclude proteinuria. An early morning sample is preferred (because it correlates best with 24-hour protein excretion) but random samples are acceptable. Urine protein excretion A 24-hour timed urine collection for protein excretion is still widely used as the reference method for comparing other ways of assessing urine. However, timed urine collections are inconvenient and not always completely accurate. However, these immunoassay methods are more expensive than those used to measure urine total protein. It is a benign condition in which proteinuria occurs only when the subjects are standing upright, and is a result of an increase in the hydrostatic pressure in the renal veins. Accuracy is further improved by measuring the urinary creatinine concentration as well and expressing the result as the protein/creatinine ratio; this corrects for Case history 12 A patient attending the hospital outpatient clinic is found to have proteinuria on dipstick testing. This leads to a relatively higher serum urea concentration than creatinine, which is not so readily reabsorbed. Metabolic acidosis: because of the inability of the kidney to excrete hydrogen ions. It usually presents as a sudden deterioration of renal function indicated by rapidly rising serum urea and creatinine concentrations. As acute renal failure is common in the severely ill, sequential monitoring of kidney function is important for early detection in this group of patients. Usually, urine output falls to less than 400 mL/24 hours, and the patient is said to be oliguric. If these pre- or post-renal factors are not corrected, patients will develop intrinsic renal damage (acute tubular necrosis). Post-renal: the urinary drainage of the kidneys is impaired because of an obstruction. Biochemical findings in pre-renal uraemia include the following: n Acute tubular necrosis Acute tubular necrosis may develop in the absence of pre-existing pre-renal or post-renal failure. Urea is increased disproportionately more than n acute blood loss in severe trauma septic shock specific renal disease, such as glomerulonephritis nephrotoxins, such as the aminoglycosides, analgesics or herbal toxins. Classification: Pre-renal Post-renal Renal Patients in the early stages of acute tubular necrosis may have only modestly increased serum urea and creatinine that then rise rapidly over a period of days, in contrast to the slow increase over months and years seen in chronic renal failure. The biochemical features that distinguish pre-renal uraemia from intrinsic renal damage are shown in Table 18. Care should be taken that the patient does not become 18 Acute renal failure Table 18. Indications for dialysis include a rapidly rising serum potassium concentration, severe acidosis, and fluid overload. An initial oliguric phase, where glomerular impairment predominates, is followed by a diuretic phase when urine output is high, as glomerular function slowly improves but tubular function remains impaired. The serum potassium usually rises very quickly in catabolic patients, with or without tissue damage, and falls quickly once the urine flow rate increases. Prompt identification of pre- or post-renal factors may allow correction of the problem before damage to nephrons occurs. Management of a patient with intrinsic renal damage will include sequential measurement of creatinine, sodium, potassium, phosphate and bicarbonate in serum, and urine sodium and potassium excretion and osmolality. Care should be taken to prevent fluid overload in the treatment of patients with renal disease. The rapidly increasing serum potassium is usually the indication to start the patient on dialysis. The end result of progressive renal damage is the same no matter what the cause of the disease may have been. The major effects of renal failure all occur because of the loss of functioning nephrons. Because of their impaired ability to regulate water balance, patients in renal failure may become fluid overloaded or fluid depleted very easily. Note that biochemical analyses have not been performed before and after all periods of dialysis. Then, a sudden deterioration of renal function may precipitate a rapid rise in serum potassium concentration. An unexpectedly high serum potassium concentration in an outpatient should always be investigated with urgency. Decreased intestinal absorption of Ca2+ Increased serum phosphate Decreased serum Ca2+ Calcium and phosphate metabolism the ability of the renal cells to make 1,25dihydroxycholecalciferol falls as the renal tubular damage progresses. The normochromic normocytic anaemia is due primarily to failure of erythropoietin production. Conservative measures may be used to alleviate symptoms before dialysis becomes necessary, and these involve much use of the biochemical laboratory. Early in chronic renal failure the normal reduction in urine formation when the patient is recumbent and asleep is lost. Patients who do not 19 Chronic renal failure and molecules move out of the blood vessels of the peritoneal wall. Note that haemodialysis and peritoneal dialysis may relieve many of the symptoms of chronic renal failure and rectify abnormal fluid and electrolyte and acidbase balance. These treatments do not, however, reverse the other metabolic, endocrine or haematological consequences of chronic renal failure. For example, ciclosporin is nephrotoxic at high concentrations and monitoring of both creatinine and ciclosporin is necessary to balance the fine line between rejection and renal damage due to the drug. Dietary sodium restriction and diuretics may be required to prevent sodium overload. Hyperphosphataemia may be controlled by oral aluminium or magnesium salts, which act by sequestering ingested phosphate in the gut. The administration of hydroxylated vitamin D metabolites may prevent the development of secondary hyperparathyroidism. Dietary restriction of protein, to reduce the formation of nitrogenous waste products, may give symptomatic improvement. The key to dialysis is the provision of a semipermeable membrane through which ions and small molecules, present in plasma at high concentration, can diffuse into the low concentrations of a rinsing fluid. In peritoneal dialysis, the dialysis fluid is placed in the peritoneal cavity, Clinical note Hypertension is both a common cause and a consequence of renal disease.
Syndromes
- Dairy
- Wear socks to bed if your feet are cold. In cold weather, wear warm socks and limit your exposure to the cold to prevent frostbite.
- If stones become infected or recur often, you may need surgery to remove the salivary gland.
- A mental disorder called psychogenic polydipsia
- Atropine
- Abnormal heart sounds or a heart murmur. These sounds may change with different body positions.
- Swollen lymph glands in the groin area
- Swallowing substances that harm the lining of the esophagus, such as household cleaners, lye, disc batteries, or battery acid
- Intestinal damage from an accident or injury
Preeclampsia was present in 28% of patients in the Boston cohort and in 12% of the patients in the study by Curry and colleagues weight loss pills during sleep 14 mg semaglutide buy with amex. Additionally weight loss medication xenical generic semaglutide 14 mg buy on-line, other medical comorbidities associated with mole-such as tachycardia and hypertension from hyperthyroidism or shortness of breath and chest pain from acute respiratory distress syndrome-may result weight loss pills zantrex 3 semaglutide 14mg order. Laboratory evidence of hyperthyroidism can occur in as many as 10% of patients; however weight loss 411 buy semaglutide 14mg low cost, clinical manifestations occur less frequently weight loss gnc semaglutide 14mg order without a prescription. Clinical manifestations of hyperthyroidism disappear once the molar pregnancy is evacuated. Antithyroid therapy may be indicated for a short period to control hyperthyroidism during molar evacuation. Other factors that may alter cardiac or pulmonary function such as preeclampsia, hyperthyroidism, and anemia are often present and more frequently contribute to acute cardiopulmonary decompensation. Respiratory distress is most often associated with a large volume of molar tissue and uterine enlargement at greater than 16 weeks gestational size. Approximately 15% to 25% of patients with unevacuated moles have theca-lutein cysts larger than 6 cm. Classically, a patient with a hydatidiform mole was said to have a uterine size excessive for gestational age. In the recent Boston study, uterine size was excessive for dates in only 28%, equal to dates in 58%, and less than dates in 14%. The later cohort had significantly less vaginal bleeding on presentation (51% vs 74%, P <0. Because molar pregnancies are diagnosed at an increasingly early gestational age, clinical symptoms are less frequent. As a result, there is increasing reliance on histopathologic analysis to identify cases of molar pregnancies. Partial moles are often underdiagnosed because of the clinical lack of suspicion and the often subtle or focal nature of the pathologic changes in the placental tissues. In a recent series based on histopathologic identification of molar pregnancies, 52% of patients were diagnosed on ultrasound examination before evacuation of the uterus. The overall detection rate was 35% to 40% before 14 weeks of gestation and 60% after. Nonetheless, less than 50% of molar pregnancies were diagnosed by ultrasound in first-trimester scans. When ultrasound was used alone, 15 (42%) of 36 patients with moles did not have a definite diagnosis on first examination. Several reports have been made of a hydatidiform mole arising in ectopic sites, such as the fallopian tube. These patients tend to present with classic symptoms and signs of ectopic pregnancy, occasionally with hemorrhagic shock resulting from tubal rupture. Histologic diagnosis of choriocarcinoma, invasive mole or placental site trophoblastic tumor 3. Usually tubal rupture occurs before the diagnostic features, suggesting molar gestation can be identified by ultrasound. Evacuation With increasing frequency, the diagnosis of mole will be made only after histologic evaluation of uterine curettings. Medical complications are observed in approximately 25% of patients with uterine enlargement at more than 14 to 16 weeks gestational size with molar pregnancy. The mole should be evacuated as soon as possible after stabilization of any medical complications. The choice of facilities for molar evacuation should be based on the expertise of the physician, uterine size, and ability of the facility to manage existing medical complications. In most patients, the preferred method of evacuation is suction dilation and evacuation (D&E) (see Table 7-2). Medical induction of labor with oxytocin or prostaglandin and hysterotomy are not recommended for evacuation because they increase blood loss and may increase the risk for malignant sequelae compared with suction D&E. The Charing Cross Group reported a significant trend toward more frequent evacuation by suction curettage compared with sharp curettage or medical induction for molar evacuation during their study interval. Furthermore, many patients require D&E to complete the evacuation of the mole after medical induction of labor. Evacuation is usually performed under general anesthesia, but local or regional anesthesia may be used for a cooperative patient with a small uterus. After serial dilatation of the cervix, uterine evacuation is accomplished with the largest cannula that can be introduced through the cervix. Intravenous oxytocin is begun after the cervix is dilated and continued for several hours postoperatively. Usually the adnexa may be preserved; theca-lutein cysts should be left in situ unless they are torsed or ruptured and actively bleeding. Hysterectomy reduces but does not eliminate the risk of malignant postmolar sequelae compared to evacuation by D&C. Efforts to correlate outcome with the histopathologic features of uterine curettings have been inconsistent, possibly because of incomplete sampling. Multiple risk factors have been incorporated into scoring systems that might identify high-, medium-, and low-risk subsets of patients. These usually contain multiple thin septations and have an appearance similar to iatrogenic ovarian hyperstimulation during ovulation induction. Of note, 144 patients were followed for less than 6 months, and another 100 were followed for up to 12 months. Prophylactic Chemotherapy after Molar Evacuation Two randomized studies have evaluated prophylactic chemotherapy after molar evacuation. In the study reported by Limpongsanurak, a single course of actinomycin-D was compared to observation in patients following evacuation of high-risk moles. However, there are anecdotal cases of fatalities caused by prophylactic chemotherapy, and prophylactic chemotherapy does not eliminate the need for postevacuation follow-up. The majority of the literature covering this relatively rare entity consists of case reports, small case series, and review of cases reported 198 7. Although there might be an increased incidence of coexisting mole and fetus related to an increase in multifetal pregnancies caused by ovulation induction for infertility, this may only reflect reporting bias. Most of these are diagnosed antepartum by ultrasound findings of a complex, cystic placental component distinct from the fetoplacental unit. However, in a few cases the diagnosis is not suspected until examination of the placenta following delivery. Medical complications of hydatidiform mole appear to be increased, including hyperthyroidism, hemorrhage, and pregnancy-induced hypertension. Among 72 patients collected by a national survey of physicians in Japan during 1997, 24 patients underwent first-trimester evacuation with 20. For patients with coexistent hydatidiform mole and fetus suspected by ultrasound, there are no clear guidelines for management. Patients are at an increased risk for medical complications of pregnancy requiring evacuation, including bleeding, premature labor, and pregnancy-induced hypertension. If fetal karyotype is normal, major fetal malformations are excluded by ultrasound, and there is no evidence of metastatic disease, it is reasonable to allow the pregnancy to continue unless pregnancy-related complications force delivery. Several classification systems have been used to determine prognostic groups and assist in the triage of management for individual patients. Invasive moles are characterized by presence of edematous chorionic villi with trophoblastic proliferation that invade directly into the myometrium. Metastasis of molar vesicles may occur, and usually invasive moles will undergo spontaneous resolution after many months, but they are treated with chemotherapy to prevent morbidity and mortality caused by uterine perforation, hemorrhage, or infection. Gestational choriocarcinomas are highly malignant, and chemotherapy is clearly indicated when diagnosed. Sheets of anaplastic polygonal cells with frequent mitoses infiltrate the smooth muscle of the uterine wall. Fortunately, most patients present with disease confined to the uterus and can be treated with hysterectomy. The index pregnancy event may have occurred years before presentation or may have been a subclinical spontaneous abortion. Before the development of effective chemotherapy, Delfs reported that of 119 patients followed after mole, 5 (4%) and 6 (5%) required hysterectomy for invasive mole or choriocarcinoma, respectively. Other prechemotherapy reports indicated a mortality rate of more than 20% among patients with invasive mole. Brewer Trophoblastic Disease Center reported their experience with 738 patients with complete hydatidiform moles. Only 15% of the 142 treated patients, or 3% of the total, developed metastases outside of the uterus. The majority of centers in the United States will also treat patients if metastases are identified. Although the overall results from this policy were excellent, outcome for patients with pulmonary metastases was not detailed. In the United States, where care is decentralized, identification of metastases is included as an indication for initiation of therapy. Although direct shunting into the systemic circulation rarely occurs, the majority of disseminated metastases develop only after pulmonary metastases have become established. The brain, liver, gastrointestinal tract, and kidneys are the distant organs most often affected, but metastases to virtually every organ have been reported. Although lymphatic spread can occur, it is relatively uncommon among patients with choriocarcinoma and invasive mole. Clinical risk factors important for assigning staging and treatment include duration of disease as determined by interval from antecedent pregnancy, type of antecedent pregnancy, and previous treatment. Because of the highly vascular nature of these lesions, biopsy is not recommended. If the vagina is the only site of metastasis, the majority of these lesions will respond to chemotherapy. A few patients will require vaginal packing or selective embolization using interventional radiology to control active hemorrhage early in the course of treatment. An ultrasound of the pelvis should also be obtained to exclude the possibility of intrauterine pregnancy before instituting chemotherapy. The clinical importance of occult pulmonary metastases is debated when they are the only sites of extrauterine metastases. However, many series of patients treated for high-risk metastases include patients who initially presented with normal chest radiographs. It would be a tragedy to miss the diagnosis of a high-risk metastasis in a patient and delay appropriate aggressive initial therapy. The experience at the University of Southern California indicated that it had an effect on the treatment in only 20% and was complicated by uterine perforation requiring hysterectomy in 8% of their patients. The Clinical Classification System, based on risk factors, has been frequently used in the United States (Table 7-5). In this system patients with nonmetastatic disease are not assigned into a prognostic group because of uniformly good outcome using simple single-agent chemotherapy. He noted survival of 70% among patients with metastatic poor prognosis disease initially treated with multiagent chemotherapy, compared to only 14% survival for patients in this category who initially received single-agent therapy. Poor tolerance of multiagent therapy was noted in the group of poor-prognosis patients receiving initial single-agent regimens, with toxicity causing death in half of these patients. Univariate analysis was used to identify prognostic factors among patients treated mainly with simple chemotherapy regimens. Others modified the weighted scoring system using a highest risk score of 6 for each prognostic factor, while not changing the total score for assigning patients into risk categories. Finally, there was no uniformity in assessing size of the largest tumor or assigning number of metastases. The Clinical Classification System had a greater sensitivity for identifying patients at risk for treatment failure and death (see Table 7-6). By multivariate analysis, both systems were roughly equivalent for stratifying patients into risk groups. Although this revised system did correlate with outcome, it resulted in a proliferation of substages of questionable importance. The total score for a patient is obtained by adding the individual scores for each prognostic factor. For these clinicians, the most important decisions revolve around identification of patients who should be referred out of the community to a specialist for treatment of high-risk disease. Because the clinical classification system (see Table 7-5) is relatively simple, it may be the best system for use by the generalist for the purpose of appropriate referral. Only four (7%) patients had disease resistant to this regimen, and three of these were salvaged with singleagent actinomycin-D. If patients have abnormal liver function, methotrexate should not be used because it is metabolized in the liver. Significant hematologic suppression, cutaneous toxicity, mucositis, alopecia, gastrointestinal toxicity, and serositis are frequently seen in patients receiving the 5-day methotrexate regimen. All patients achieved sustained remission but 51% required a second drug, 14% needed combination chemotherapy, and 12% required surgery to remove drug-resistant disease. Patients were treated with actinomycin-D for documented methotrexate resistance or toxicity with equal frequency. Overall, 78% achieved remission using the primary regimen with or without hysterectomy; all eventually achieved remission, and only one (1. Whereas toxicity sparing may be true for high doses of methotrexate, Rotmensch and associates evaluated methotrexate levels in patients after daily methotrexate therapy compared to levels in patients receiving alternating daily doses of methotrexate and folinic acid, with a higher daily dose of methotrexate given in the methotrexate/folinic acid regimen. They noted that whereas patients on the methotrexate/ folinic acid regimen had higher peak methotrexate levels after treatment with a higher methotrexate dose than those on single-agent methotrexate, trough levels were both subtoxic and subtherapeutic 24 hours after methotrexate administration.
Cheap semaglutide 14 mg overnight delivery. 5 Kg Weight Loss in 1 Week with Turmeric Tea | Weight Loss Recipes of Turmeric Detox Tea | Hindi.
References
- Gammon GD, Burge FW, King G. Neural toxicity in tuberculous patients treated with isoniazid (isonicotinic acid hydrazide). AMA Arch Neurol Psychiatry. 1953;70:64-69.
- Diener HC, for the ASASUMAMIG Study Group. Efficacy and safety of intravenous acetylsalicylic acid lysinate compared to subcutaneous sumatriptan and parenteral placebo in the acute treatment of migraine. A double-blind, double-dummy, randomized, multicenter, parallel group study. Cephalalgia 1999; 19:581-8.
- Williams, M.A., Giel, D.W., Colleen Hastings, M. Endoscopic Deflux injection for pediatric transplant reflux: a feasible alternative to open ureteral reimplant. J Pediatr Urol 2008;4:341-344.
- Milgrom SA, Kollmeier MA, Abu-Rustum NR, et al. Quantifying the risk of recurrence and death in stage III (FIGO 2009) endometrial cancer. Gynecol Oncol 2014;134(2):297-301.