
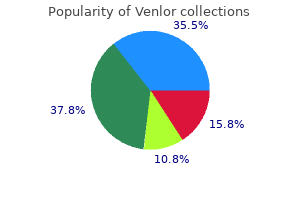
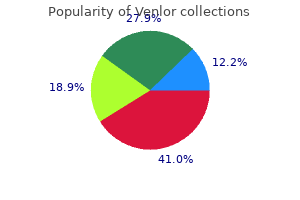
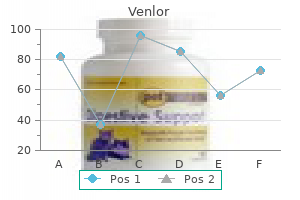
Venlor
| Contato
Página Inicial
Alan Jay Schwartz, MD, MSEd
- Professor
- Clinical Anesthesiology and Critical Care
- University of Pennsylvania School of Medicine
- Director of Education and Program Director
- Pediatric Anesthesiology Fellowship
- Department of Anesthesiology and Critical Care Medicine
- Children's Hospital of Philadelphia
- Philadelphia, Pennsylvania
Comparison of the analgesic efficacy and respiratory effects of morphine anxiety symptoms knot in stomach best 75 mg venlor, tramadol and codeine after craniotomy anxiety statistics purchase genuine venlor on-line. Regional scalp block for postcraniotomy analgesia: a systematic review and meta-analysis anxiety symptoms depersonalization venlor 75 mg order amex. Over the last 3 decades anxiety symptoms out of the blue purchase venlor 75 mg with amex, lumbar spinal fusion rates have risen dramatically anxiety symptoms one side cheap venlor 75 mg buy line, with rates increasing 2-fold in the 1980s, 3-fold in the 1990s, and 2. These cases are frequently performed on and near vital structures and in the prone or lateral position, making airway edema and positioning injuries more likely. The highest rate of increase in spinal fusion surgery has been in patients over the age of 60 years who have more comorbidities and experience higher complication rates. This article is geared toward the neurointensivist and divided into subheadings discussing complications or issues related to all spine procedures as well as a focus on site-specific complications. Preoperative planning before spine surgery can be helpful in optimizing patients for surgery and managing postoperative expectations. Many hospitals have developed clinical pathways for spine surgery, which can involve a multidisciplinary team of physical therapists, nutritionists, and pain management physicians who help with planning for preoperative and postoperative therapies. Patients taking opioid medications prior to surgery may have increased opioid requirements postoperatively. A study of spine surgery patients found that 20% were opioid dependent, with the highest rates in lumbar decompression and fusion cases (23. This can be particularly problematic with the high rates of obesity in spine patients and associated obstructive sleep apnea. Goals for the management of acute spinal cord injuries include limiting secondary injury and maximizing spinal cord perfusion. Neurogenic shock can cause hemodynamic instability, resulting in bradycardia, cardiac dysfunction, hypotension, and decreased systemic vascular resistance and often requires atropine, volume resuscitation, and vasopressor/inotropic support to maintain spinal cord perfusion. For minor operative procedures in areas at low risk for hemorrhage, transfusion is rarely required in the operating room. Preoperative hematocrit levels of greater than 21% may provide a margin of safety. Coagulopathy in major spine surgery can be very detrimental because there are large surfaces of decorticated bone that can be difficult to completely cauterize. In this regard, many anesthesiologists administer antifibrinolytics during the procedure in addition to optimizing the international normalized ratio and platelet count. Antifibrinolytics have been shown to decrease total blood loss and transfusions during spine surgery. Although they do not appear to increase the risk of thrombotic events, caution is warranted in patients at high risk for clotting. The neurocritical care unit may manage spine patients both preoperatively and postoperatively. Knowledge of the procedure and potential complications will enable the intensivist to better prepare the patient for surgery. Patients who are cared for in the neurocritical care unit preoperatively prior to major spine surgery may have associated major traumatic injuries, acute lung injury, acute spinal cord injury, and/or a traumatic brain injury. Stabilizing the spine in trauma patients is critical for optimal mobilization, and surgery should be done as soon as is safely possible. Careful neurological examination of patients immediately prior to their operative interventions is important to provide a baseline neurological assessment so that any new neurological injuries postoperatively may be Perioperative Concerns in Management of Patients Undergoing Spinal Surgery Key Concepts Fluid management should be goal directed to maintain euvolemia. A detailed conversation preoperatively with the anesthesiologist regarding the patient will ensure good transition of care. The large venous channels in the thoracolumbar spine, the numerous vertebral levels involved in these procedures, and the high number of pedicle screws inserted may explain their frequency in these procedures. One study utilizing transesophageal echocardiography in the prone position found an 80% incidence of moderate- to high-grade emboli in instrumented spines, particularly during pedicle screw insertion. Most patients do not have obvious hemodynamic effects from these thousands of microemboli, but it is possible that they contribute to surgical inflammation and other complications. Conservative management or postponement of surgery should be considered for patients with poorly controlled intracranial hypertension or extremely tenuous cardiopulmonary conditions. An important consideration in evaluating effects of prone positioning is the integrity of the airway. Use of some prone pillows can predispose to endotracheal tube kinks with associated airway obstruction. Prone patients in pins or prone head rests may be susceptible to inadvertent extubation. Most anesthesiologists pay extra attention to securing the airway with tape and securing the breathing circuit to the bed or head frame to avoid tension on the airway. Acute kidney injury if relative hypovolemia and hypotension persist Inadequate oxygenation and ventilation from high intrathoracic pressure Oxygenation typically improves in the prone position if adequate tidal volumes can be achieved Elevated intracranial pressure with poor intracranial compliance. Operative duration as an independent risk factor for postoperative complications in single-level lumbar fusions. Facial and Oropharyngeal Edema Requiring Postoperative Mechanical Ventilation Edema of the face and oropharynx can occur after procedures done in the prone position. This is especially true for longer cases in which greater amounts of intravenous fluids are administered. Checking for leaks around the endotracheal tube with the cuff deflated can also be done, with lesser leaks being more predictive of postextubation stridor and increased risk of reintubation. Injuries to the brachial plexus can also occur from direct compression from chest supports. Areas at risk in the prone position include the forehead, chin, cheeks, nose, tongue, chest, and iliac crests. Padding some of these skin areas at risk may reduce the risk of pressure sores, but definitive data are lacking. Its diagnosis, risk factors, and workup are discussed in more detail at the end of this chapter. Knowledge of the most common types of complications in spine surgery patients informs the entire perioperative management with preventative measures and heightened scrutiny preoperatively, intraoperatively, and postoperatively. Many of these complications will be discussed in further detail in subsequent chapters covering different approaches to the spine (Chapters 3133). Risk factors from one study included surgical duration more than 5 hours, blood loss more than 300 mL, surgery on C4 or higher, and more than three levels of exposure. Specific Operative Procedures and Complications Key Concepts the overall complication rate in all spinal fusion procedures is approximately 10%, but certain procedures, such as major spinal reconstruction for scoliosis, may have complication rates as high as 61%. Anterior cervical spine surgery is a commonly performed procedure used to treat a wide variety of cervical pathologies. Anterior cervical spine procedures carry a relatively low complication rate of approximately 3%, with the exception of dysphagia, which is very common in these procedures. For nonoperative site injuries, evaluation by a neurologist should occur as early as possible. Electrophysiological testing may be done; however, it may have to be delayed several weeks to ensure accuracy. Consultation with an otolaryngologist can be helpful in diagnosing vocal cord dysfunction. If present, evaluation of speech and swallowing should be done to minimize the risk of aspiration. Patients with significant respiratory compromise should be reintubated and may require tracheostomy if bilateral nerve injuries are present. Hematomas can expand quickly and cause distortion of the anatomical structures, which can make airway management more difficult. The incidence of hematomas after anterior cervical discectomy and fusion surgery ranges from 0. Mean time to symptom onset was 24 hours for patients requiring reintubation in the first study, and an average of 3 hours to reintubation in the second. Risk factors for airway complications were operative duration more than 5 hours; blood loss greater than 300 mL; exposure of more than three vertebral levels; or surgery on C2, C3, or C4 in the first study and preoperative myelopathy and multilevel corpectomy in the second. Note the numerous structures at risk for injury, including the carotid artery, internal and external jugular veins, pharynx, esophagus, recurrent laryngeal nerve, pleura, and others. Opening the neck at the bedside will relieve pressure from a rapidly expanding hematoma but may be less helpful for edema or a hematoma tracking cephalad. Awake or asleep intubation with a variety of airway devices, including direct laryngoscopy, may be utilized depending on the situation and degree of airway compromise. A similar level of support may be considered when extubating such patients in the context of lack of certainty regarding success of extubation. Pharyngeal and Esophageal Perforations Pharyngeal and esophageal perforations are rare but potentially fatal complications of anterior cervical spine surgery that can result in pneumothorax, mediastinitis, sepsis, and respiratory failure. The three most common signs and symptoms are dysphagia, neck abscess, and aspiration pneumonia. A recent literature review found that 1% to 79% of patients have dysphagia in the first week after surgery, 50% to 56% at 1 month, and 8% to 21% at 6 months. Swallowing evaluations should be obtained for more clinically symptomatic cases to reduce the risk of aspiration. In some cases tube feeding is indicated postoperatively, and if intractable and severe, a gastrostomy may be needed. Surgery on the thoracic and lumbar spine can be approached posteriorly, anteriorly, or laterally. Injury to large vessels such as the iliac arteries and veins, bowel, pleura, and other structures can result in life-threatening complications. The overall incidence for neurological injury after posterior cervical spine fusion is 0. Vertebral Artery Injuries Injury to the vertebral artery during cervical spine surgery can be devastating and lead to severe problems such as fistulas, pseudoaneurysm, dissection, bleeding and thrombosis, embolism, cerebral ischemia, and even death. Stroke from this complication generally involves the posterior circulation and thus can lead to issues related to brainstem or occipital cortex function. Anticoagulation and antiplatelet therapy may also be needed to help prevent thromboembolic events. Blood Loss Blood loss can be significant regardless of approach and can continue into the postoperative period. Although major vascular injuries are rare with anterior lumbar procedures, blood loss will be rapid and difficult to control if the iliac vessels are injured. Posteriorly, epidural venous bleeding is one of the more common causes of rapid blood loss. Certain aspects of these operations, such as costotransversectomies and osteotomies, have the potential for greater blood loss because of segmental intercostal vessels and the complex system of venous drainage of the vertebrae. Anterior or anterolateral approaches to low cervical or high thoracic vertebrae are at risk for injury to the major vascular structures in the neck and chest. Postoperative Neurological Complications and Causes for Reoperation Worsened myelopathy may be present in up to 4% of these procedures. These deficits may resolve without reoperation; however, some patients may need to return to the operating room for repositioning of the hardware. Pedicle screws may also need to be repositioned because of their proximity to major blood vessels such as the aorta. Rod or pedicle screw breakage or loosening is common in the first 2 years postoperatively and can require reoperation. Rapidly evolving neurological deficits within or near the operative site should raise alarm for a potential epidural hematoma (see section on epidural hematoma later in this chapter for workup). Decisions regarding power of attorney, advanced directives, and do not resuscitate orders should be solicited regardless of treatment choice. Some patients will require a staged spine procedure performed on separate days, typically because of an expected prolonged procedure with high blood loss or a combined anterior and posterior approach to the spine. If the procedure is done in a staged fashion, the patient may require postoperative controlled ventilation between stages if the interval between operations is very short. Varied results have been obtained for complication rates related to staging major spinal procedures. An analysis of 11,265 patients who underwent circumferential spine surgery48 showed that the overall complication rate was significantly higher in patients undergoing staged versus same-day procedures with overall complication rates of 28. These data were taken from a national database, and it is unclear if the staged procedures were planned or performed because of life-threatening complications. In contrast, other studies either reported no difference in complications between staged and unstaged procedures46 or found that staging anterior-posterior procedures more than 21 days apart decreased transfusion requirements and improved patient functionality. However, if intraoperative patient condition is rapidly deteriorating and cannot be corrected with respect to blood loss, coagulopathy, acidosis, hypotension, and other physiological parameters, staging the procedure may be a lifesaving maneuver. These patients may require large amounts of fluids and blood products intraoperatively, and resuscitation may continue well into the postoperative period. Special attention to the intraoperative blood loss and postoperative losses through drain output will be needed. Frequent laboratory assessment of hematocrit, coagulation parameters, and acidbase status with attention to the hemodynamic condition can help guide resuscitation efforts. A more detailed review of the approach to postoperative management of exsanguination is reviewed in Chapter 7. Immediate diagnosis and decompression are needed to minimize spinal cord injury related to expanding hematoma. It is considered a surgical emergency and thus warrants frequent neurological assessment postoperatively. Signs and symptoms can include a spectrum from inordinate surgical site pain to paresis to paralysis. Time to decompression correlates with neurological recovery, with better outcomes for symptom-to-decompression times of 6 to 8 hours. Elderly patients with cervical spine fractures sustained after a fall from standing have a very high complication rate (62%) and early mortality rate (13%).
There is a 15% incidence of postoperative seizures after cranioplasty performed to repair skull defects after decompressive craniectomy anxiety symptoms change over time buy venlor 75 mg free shipping. In a series of 36 such patients anxiety symptoms for hiv generic 75 mg venlor visa, 7 had immediate seizures anxiety symptoms heart palpitations purchase 75 mg venlor visa, 2 had early seizures anxiety 4 days after drinking buy venlor 75 mg otc, and 27 had late-onset seizures (after 7 days) anxiety level test discount venlor american express. In those with cerebral abscesses the incidence of late, unprovoked postoperative seizures with many years of follow-up is 92%. In general, the risk of developing seizures decreases with the passage of time after surgery, with the risk of developing new seizure activity falling to less than 10% by 6 months,25 although patients with surgically treated abscesses have a risk of developing new seizures that persists after 5 years. A study of 877 patients in a neurosurgical center in the United Kingdom in the early 1970s (none with prior history of epilepsy) who underwent supratentorial neurosurgery reported that 17% developed postoperative seizures. Of those who had postoperative seizures, 77% occurred within 1 year and 92% occurred within 2 years. For those with mild head injury, the increased risk compared with the general population persisted for 5 years but not thereafter. Increased number of operative interventions in the management of trauma is correlated with increased risk of late posttraumatic seizures. Prophylaxis or treatment of early posttraumatic seizures is not known to influence the subsequent development of posttraumatic epilepsy or any other outcome measure. However, it is clear from many studies that longer prophylaxis (>12 weeks) does not prevent or delay late seizures or epilepsy, but does expose the patients to possible adverse effects and probably decreased rehabilitation potential. Prophylaxis Key Concepts the purpose of prophylactic treatment is to prevent immediate and early postoperative seizures-it does not reduce the risk of late seizures. There is a paucity of randomized, controlled trials for seizure prophylaxis postcraniotomy. For instance, lamotrigine and felbamate have neuroprotective effects in experimental animals. For example, in patients with cerebral neoplasms, it is often better to avoid strong P450 enzyme inducers such as phenytoin, carbamazepine, phenobarbital, and primidone because they can lower the efficacy of steroids and chemotherapeutics. In routine brain surgery for resection of tumors without prior seizures, the risk is low and prophylaxis is of questionable benefit. A newer agent so does not have as robust data as phenytoin Clinical Pearl Patients who develop seizures in the immediate or early postoperative period do not necessarily have a liability to further seizures and do not warrant long-term prophylaxis. It is not recommended in patients after subarachnoid hemorrhage given its cognitive effects. In a hemodynamically unstable patient-such as after an operation with significant blood loss-it is important to be aware of this possibility and either be prepared to address blood pressure lability on an emergent basis or consider an alternative agent. Phenytoin Phenytoin has long been the standard for postoperative seizure prophylaxis. It is well studied, inexpensive, widely used, does not compromise level of consciousness, and is available intravenously. It is often the "gold-standard" comparison arm in trials of postoperative seizure prophylaxis. The rationale for its use postoperatively is partially extrapolated from its use in the prevention of late posttraumatic seizures. This trial exclusively concerned patients requiring elective craniotomy for supratentorial brain tumors and excluded patients with seizures in the 7 days prior to surgery, although 30% of both the treatment and control groups had a prior history of seizures at some point. On the day of surgery, a loading dose of 18 mg/kg of phenytoin was administered (this is in line with prior dosing regimens57), and administration continued for 7 days with a goal total serum concentration of 10 to 20 g/mL. Thirteen percent of the treatment group experienced early seizures and 11% of the control group experienced them. This study was significant in that it exclusively concerned cases of brain tumor resection and did not include cases of head trauma (it is known independently that phenytoin can prevent early seizures in that population49). Although its side effect profile is acceptable with short-term use only,58 there is likely no role for phenytoin in the prevention of early postoperative seizures in those undergoing craniotomy for supratentorial tumor resection. Its favorable pharmacokinetic profile makes it attractive for use in those undergoing concomitant chemotherapy for malignant neoplasms, and it may be substituted for phenytoin in the postoperative period. Patients found to have contraindications to phenytoin (including depressed left ventricular ejection fraction, cardiac arrhythmias, or hypotension) were instead administered levetiracetam. In this study, 9/210 patients taking phenytoin had a seizure within 7 days, whereas only 1/105 patients taking levetiracetam had a seizure within 7 days (however, the difference between these two agents did not attain statistical significance: p ¼ 0. Of note, however, adverse reactions were far less prevalent in those taking levetiracetam (p <0. The relationship between levetiracetam and possible emergence delirium is not known. It should be noted that this was a small, retrospective trial with an older population of patients in the phenytoin group. One trial of 63 patients operated on for supratentorial neoplasms randomized patients to receive phenobarbital (4 mg/kg intravenously for 5 days followed by an oral switch) or phenytoin (10 mg/kg intravenously for 5 days followed by an oral switch) and suggested that they were equivalent in efficacy. They failed to show a benefit over a 6-month period in terms of seizure occurrence. Like phenytoin, carbamazepine is not known to exert an antiepileptogenic effect in experimental animals. Valproic Acid Valproic acid has been studied extensively for treatment of the epilepsies and posttraumatic seizures and for seizure prophylaxis in patients with intracranial malignancies. With respect to postoperative seizure prophylaxis, its tendency to cause thrombocytopenia, platelet dysfunction, hypofibrinogenemia, and other bleeding tendencies is at least a theoretical concern. However, fewer patients being treated with valproate stopped treatment due to adverse effects. There was no difference in the rate of early or late postoperative seizures between those treated with phenytoin versus valproate. However, there was no difference in the rate of coagulopathies between the two drugs. It does not have a role in primary seizure prophylaxis in newly diagnosed intracranial tumors. Oxcarbazepine Oxcarbazepine has not been used widely in management of postoperative seizures. One hundred fifty patients were treated with 900 to 1200 mg oxcarbazepine daily in two divided doses starting 7 days prior to surgery. There was no comparison with placebo or standard of care in this preliminary study. One must be particularly vigilant to the possibility of hyponatremia, which is even more common with oxcarbazepine than with carbamazepine and can be an important issue in neurosurgical patients. Management Key Concepts Status epilepticus is defined as continuous seizures that last longer than 5 minutes or recurrent seizures without recovery of mental status between seizures. In this section we will address the management of seizures that arise in the early postoperative period, including those that progress to status epilepticus, with emphasis on considerations specific to the postoperative patient. Although postoperative seizure liability can be expected to arise from cortical irritation at the site of operation, there are multiple other factors around surgery that can predispose to seizure activity, particularly in a vulnerable host. Consideration should be given not only to surgical complications (such as intracranial bleeding or hematoma formation), but also anesthetic and metabolic factors (such as hyponatremia that might occur in cerebral salt wasting syndrome) or the syndrome of inappropriate antidiuretic hormone secretion. Continuous vital sign monitoring (heart rate, blood pressure, respiratory rate, oxygen saturation, and temperature) 4. The goal for those who have responded to emergent initial therapy is to obtain therapeutic concentrations in the bloodstream in advance of continuing maintenance therapy. For those who have not responded to emergent initial therapy, its role is to terminate seizure activity. Treatment of refractory status epilepticus (which occurs in 40% of cases of status epilepticus):72 A. It is recommended that the level of anesthesia is titrated such that there is no evidence of electrographic seizures but not necessarily to a level that produces the so-called suppression-burst pattern. There is no evidence to support a particular hematocrit goal in status epilepticus. However, in the critical care literature in general, a majority of studies favor a conservative transfusion strategy over a liberal one. However, nonconvulsive seizures are a common, underrecognized phenomenon in hospitalized patients and are associated with worse outcomes. However, the nonconvulsive form does not have the same systemic physiological perturbances as the convulsive status epileticus. However, the majority of seizures in hospitalized patients, including the critically ill, are nonconvulsive. Clinical Pearl After generalized convulsive status epilepticus, 48% of patients will have nonconvulsive seizures within the next 24 hours. Clinical Pearl Nonconvulsive seizures should always be considered if a patient remains persistently altered >10 to 30 minutes after convulsions cease. The clinical manifestations, if any, are variable and include subtle changes in behavior, face and limb myoclonus, eye deviation, autonomic instability, or delayed emergence from anesthesia. Long-term monitoring is necessary because a short course will miss over half of cases. Immediate and early postoperative seizures occur due to tissue trauma with consequent free radical generation, neuronal hyperexcitability due to disturbance of the ionic milieu across the cell membrane, and alterations in the function of inhibitory interneuron function. The incidence of postoperative seizures varies between 17% and 37% across studies (and is up to 92% for certain subgroups of patients). The liability to seizure activity can be risk stratified based on the indication for surgery, operative approach, location, and type of surgery. Anesthetic care during thiopental tests to evaluate epileptic patients for surgical therapy. The neuropathologic effects in rats and neurometabolic effects in humans of large-dose remifentanil. A retrospective comparison of remifentanil versus methohexital for anesthesia in electroconvulsive therapy. Do prophylactic anticonvulsant drugs alter the pattern of seizures after craniotomy Incidence of postoperative epilepsy in children following subfrontal craniotomy for tumor. Seizure outcome in patients with surgically treated cerebral arteriovenous malformations. Practice parameter: antiepileptic drug prophylaxis in severe traumatic brain injury: report of the Quality Standards Subcommittee of the American Academy of Neurology. Anti-epileptic drugs for preventing seizures following acute traumatic brain injury. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Prophylaxis against postoperative seizures is not indicated routinely in patients postcraniotomy; however, given the low morbidity associated with at least a short course of an antiepileptic agent, it is common practice. Prophylaxis is reasonable for high-risk subgroups of patients during the acute setting only; high-risk generally refers to a patient deemed to have at least a 10% to 15% chance of early postoperative seizures. The most well-studied agent for prophylaxis is phenytoin, but levetiracetam seems to be as effective and better tolerated. Other agents exist, and choice of agent should depend on individual patient factors. The management of postoperative status epilepticus has a number of considerations in postneurosurgical patients because the underlying etiology is likely to be different than in a nonsurgical host. However, the fundamental principles are the same: airway stabilization, optimization of hemodynamic parameters, promoting optimal gas exchange, and addressing the underlying cause while implementing a logical, stepwise approach to emergent pharmacotherapy. Preoperative and postoperative seizures in patients with astrocytic tumours: analysis of incidence and influencing factors. Epilepsy after craniotomy and the place of prophylactic anticonvulsant drugs: discussion paper. Acute seizures after intracerebral hemorrhage: a factor in progressive midline shift and outcome. Analyzing risk factors for late posttraumatic seizures: a prospective, multicenter investigation. Natural antioxidants may prevent posttraumatic epilepsy: a proposal based on experimental animal studies. Free radical production correlates with cell death in an in vitro model of epilepsy. Antiepileptogenesis and seizure prevention trials with antiepileptic drugs: meta-analysis of controlled trials. An electrophysiological analysis of the protective effects of felbamate, lamotrigine, and lidocaine on the functional recovery from in vitro ischemia in rat neocortical slices. P450 enzyme inducing and non-enzyme inducing antiepileptics in glioblastoma patients treated with standard chemotherapy. Clinically important drug interactions in epilepsy: general features and interactions between antiepileptic drugs. Compare ative double blind clinical trial of phenytoin and sodium valproate as anticonvulsant prophylaxis after craniotomy: efficacy, tolerability, and cognitive effects. Prophylactic effects of phenytoin, phenobarbital, and carbamazepine examined in kindling cat preparations. Side effects and mortality associated with use of phenytoin for early posttraumatic seizure prophylaxis. Safety and feasibility of switching from phenytoin to levetiracetam monotherapy for glioma-related 507 61. A retrospective two-center study of antiepileptic prophylaxis in patients with surgically treated high-grade gliomas. Efficacy and tolerability of levetiracetam versus phenytoin after supratentorial neurosurgery. Pharmacological management of seizures and status epilepticus in critically ill patients. Influence of surgery and antiepileptic drugs on seizures symptomatic of cerebral tumours.
He was found to have degenerative lumbar scoliosis (A) and underwent a lateral approach for decompression and interbody fusion anxiety symptoms worksheet buy venlor on line amex. The patient underwent a second-stage posterior decompression and fusion with pedicle screws anxiety medicine for dogs purchase venlor 75 mg on line. Most patients experience a nearcomplete recovery of this deficit by 1 year after surgery anxiety medicine for dogs discount venlor 75 mg buy online. For those patients in whom the psoas muscle was entered anxiety chest pain generic venlor 75 mg buy line, a transient mild hip flexion weakness may exist because the muscle has been damaged anxiety symptoms hot flashes purchase venlor online pills. However, this is not considered a complication unless it is accompanied by knee extension weakness, which is indicative of a femoral nerve injury. The chest tube(s) are removed after output has decreased and chest x-rays are stable, generally after 24 to 48 hours if there is no air leak. Prolonged lateral positioning can be associated with significant dependent skin breakdown, nerve palsies, and dependent lung edema. Clinical Pearls the postoperative ileus rate appears to be higher from a transperitoneal versus a retroperitoneal approach. Drains that communicate with the peritoneal space can have substantial sustained output. This does not necessarily imply pathology but may just reflect physiological peritoneal fluid. If nausea or radiographic enlargement of bowel loops is evident, then placement of a nasogastric tube may be necessary. Transthoracic Approaches Many complications from a thoracotomy are decreased by appropriate preoperative workup for comorbidities, such as cardiac or pulmonary disease. Regardless, the possibility of certain complications must be considered in the perioperative period38,39 (Table 33. A lung laceration may occur during dissection of pleural adhesions or from direct trauma with an instrument, thereby increasing risk for postoperative pneumothorax. After repair, a chest tube is placed near the location of potential air leak, biased anteriorly in the chest to account for anterior migration of air within the thoracic cavity. Chylothorax is identified by postoperative chest x-ray, combined with a milky fluid emission from the chest tube. Thoracentesis or repeat thoracotomy for further repair remain options for continued chyle output. If early in development, chest tube drainage with intravenous antibiotics may successfully treat the process. Late-stage pleural abscess may require thoracotomy for decortication and evacuation. This can result in significant intraoperative blood loss requiring aggressive intraop and postoperative resuscitation. In the case of a postoperative pneumothorax, an anteriorly placed chest tube should remain in place until the pneumothorax resolves. Pneumothorax recurrences are treated by numerous methods, including observation, replacement of chest tube, or repeat thoracotomy with placement of chest tube. Signs of tension pneumothorax include respiratory distress, hypoxemia, decreased unilateral lung sounds, tracheal deviation, distended neck veins, hypotension, and tachycardia. Lacerations of thoracic vessels are managed by either ligation of the vessel or with primary repair, but still increase the risk for postoperative complications. The azygos vein and segmental vessels can often be ligated in the case of laceration. If laceration of the inferior vena cava occurs, primary repair is attempted, but ligation remains an acceptable damage control technique. Superior vena cava ligation can produce acute superior vena cava syndrome and jeopardize vision. If bleeding is expected in the postoperative period, the chest tube should be placed in the anticipated location of blood accumulation (often oriented posteriorly in the paraspinous region). If high output continues or increases, then consideration for repeat thoracotomy and direct hemostasis should be given. If the peritoneum is violated and not repaired at the time of surgery, a hernia, and possibly bowel obstruction or infarction, can occur. Injury to the bowel is a rare complication requiring immediate detection and treatment. Preoperative bowel prep and intraoperative nasogastric tube insertion can decrease the risk of the complication by decompressing loops of bowel. Appropriate vascular access and readily available blood products should be present in preparation for this potential complication. If it arises, postoperative issues related to massive transfusion and ongoing hemorrhage may arise. However, it is very difficult to control because access to the thecal sac is limited. Free muscle or fascia grafts should be harvested and may be combined with a fibrin glue to promote healing. A lumbar subarachnoid drain should be inserted to divert cerebrospinal fluid in the immediate postoperative course. If hematoma, retropulsed disc material, or malpositioned hardware is causing compression, dorsal decompression and exploration is the most efficacious treatment strategy. These nerve palsies typically resolve spontaneously within the first 6 months after surgery. This complication may result in ipsilateral vasodilatation in the lower extremity vessels. The patient will usually complain, though, of a cold sensation in the contralateral foot. There is no surgical management strategy for this complication, but 25% to 33% of patients recover normal function by 2 years. If there is an epidural component causing compression of the neural elements, ventral or dorsal exploration and debridement is recommended. Otherwise, prolonged antibiotic use with an external orthosis may be attempted with radiographic and clinical surveillance. Anterior transsternal approach for treatment of upper thoracic vertebral tuberculosis. Lateral extracavitary, costotransversectomy, and transthoracic thoracotomy approaches to the thoracic spine: review of techniques and complications. Thoracic disc disease: experience with the transpedicular approach in twenty consecutive patients. Thoracoscopic approaches to the thoracic spine: experience with 241 surgical procedures. Anterior single rod instrumentation for thoracolumbar adolescent idiopathic scoliosis with and without the use of structural interbody support. Adolescent idiopathic scoliosis treated with open instrumented anterior spinal fusion: five-year follow-up. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Thoracolumbar spine trauma classification: the Thoracolumbar Injury Classification and Severity Score system and case examples. Surgical management and clinical outcomes of multiple-level symptomatic herniated thoracic discs. Blood supply and vascular reactivity of the spinal cord under normal and pathological conditions. This complication can be avoided with vigilant neuromonitoring and stimulating the region exposed within the retractor blades in search of motor nerve branches. Usually this complication is purely esthetic, but can be very troubling to patients. Conclusion Through multidisciplinary care from the spinal surgeon and the neurocritical care specialist, patients undergoing transthoracic or transabdominal spinal surgery can achieve optimal outcomes. Specifically, vigilant postoperative care, often in the intensive care unit, is necessary for the identification and management of potential complications. Medical complications of surgical treatment of adult spinal deformity and how to avoid them. Treatment strategy for chylothorax after pulmonary resection and lymph node dissection for lung cancer. Visceral and vascular complications resulting from anterior lumbar interbody fusion. Comparison of conventional versus minimally invasive extraperitoneal approach for anterior lumbar interbody fusion. Motor nerve injuries following the minimally invasive lateral transpsoas approach. Cord monitoring changes and segmental vessel ligation in the "at risk" cord during anterior spinal deformity surgery. Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2004. Indications and results of combined anterior-posterior approaches for spine tumor surgery. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Surgical decision making for unstable thoracolumbar spine injuries: results of a consensus panel review by the Spine Trauma Study Group. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: a radiographic study. Early outcomes and safety of the minimally invasive, lateral retroperitoneal transpsoas approach for adult degenerative scoliosis. Dynamically evoked, discrete-threshold electromyography in the extreme lateral interbody fusion approach. Minimally invasive lateral transpsoas approach with advanced neurophysiologic monitoring for lumbar interbody fusion. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Smoking and timing of cessation: impact on pulmonary complications after thoracotomy. At this point, communication with the anesthesia team is critical because balloon inflation often induces transient bradycardia, necessitating treatment with an anticholinergic agent such as glycopyrrolate. Once the balloon is deflated and removed, a stent is then guided over the wire and deployed within the area of previous stenosis. Neuroanatomy and Procedure Key Concepts Balloon angioplasty and stenting are commonly performed to treat patients with cervical internal carotid artery stenosis. The trial was stopped early due to higher 30-day stroke or death rate in the interventional group (14. Of the hemorrhagic strokes, four were due to vessel ruptures likely from microwire perforations and five were thought to be reperfusion hemorrhages. Of the ischemic strokes, most were considered perforator infarcts from the basilar artery. Typically a 6 French sheath is placed in the femoral artery and, under fluoroscopic guidance, a guide catheter is navigated into the cervical internal carotid or vertebral artery. At this time, heparin is administered intravenously to achieve an activated clotting time of >250. Next, a noncompliant balloon microcatheter is navigated over a microwire across the area of stenosis. Under fluoroscopic guidance, the balloon is inflated to a nominal pressure to expand the area of stenosis. Next, after the balloon microcatheter is withdrawn, a separate microcatheter is navigated beyond the area of stenosis. As the microcatheter is withdrawn, the stent is "unsheathed" across the area of previous stenosis. Contrary to its use for stenosis, intracranial stent placement for assistance in elective treatment of brain aneurysms is very common. This stent-assisted coil technique has been shown to achieve a high rate of long-term aneurysm occlusion with a very acceptable risk profile in patients undergoing elective treatment for aneurysms. Angiogram post stent-assisted coil embolization shows exclusion of the aneurysm with minimal filing at the aneurysm base. This is a stentlike device constructed of a fine network of cobalt and chromium mesh resulting in 30% to 35% metal surface area coverage. Although these devices provide a welcome treatment option for extremely challenging aneurysms with a poor natural history and paucity of other safe and effective treatments, the risk of adverse event may be higher than with traditional endovascular techniques for simpler aneurysms. The technique for deployment of these devices is similar to those for intracranial arterial angioplasty and stenting; however, no balloon angioplasty is performed. Additionally, for specific cases, two microcatheters are placed within the guide catheter simultaneously in order to performing a "jailing" technique. This includes navigating the first microcatheter into the aneurysm neck, where it will remain while the stent is deployed through the second microcatheter. This enables the first microcatheter to already be in optimal position for coiling as opposed to subsequently navigating that catheter through the stent tines into the aneurysm neck. These procedures are also routinely performed with the patient fully anticoagulated with heparin. Angiogram postdeployment of Pipeline embolization device shows reduction in filling of the aneurysm (E) with expected stagnation within aneurysm as seen on unsubtracted image (F; Pipeline device outlined by curved line). Perioperative Considerations Key Concepts Maintaining hemodynamic stability while stenting is important and may require anticholinergic agents or pressors.
This may be a consideration for nonhemodialysis patients with limited access to a healthcare facility to receive intravenous iron anxiety keeping me awake purchase venlor 75 mg mastercard, and it preserves veins for future hemodialysis vascular access because fewer infusions are required anxiety vertigo 75 mg venlor purchase. Iron sucrose and iron gluconate have never been associated with a fatal anaphylactic reaction and do not require a test dose anxiety questionnaire generic venlor 75 mg visa. However anxiety 4 year old buy venlor 75 mg low price, they can be administered to a maximum of only 250 to 300 mg per session anxiety urination purchase online venlor, so a nonhemodialysis patient with severe iron deficiency will require several infusions to replete iron stores. Iron sucrose and iron gluconate are preferred in patients undergoing hemodialysis whose regular visits and access to the circulation through the extracorporeal circuit make smaller and more frequent dosing appropriate. Iron sucrose and iron gluconate have been associated with nonfatal anaphylactic reactions, hypotension, and nausea/vomiting. For iron dextran, sucrose, and gluconate, slower infusion rates and smaller doses in a single session are associated with a lower incidence of side effects. There are two intravenous iron preparations, ferumoxytol and ferric carboxymaltose, that can be given in infusion doses of 510 and 750 mg, respectively. A second 750-mg dose of ferric carboxymaltose can be administered at least 7 days later for a maximum cumulative dose of 1500 mg per course. The safety profiles of ferumoxytol and ferric carboxymaltose appear to be similar to those of iron sucrose and gluconate, with serious adverse events occurring in 0. Characteristics of available intravenous iron preparations are summarized in Table 56. It is undergoing phase 3 trials in the United States 522 Section10-chronicKidneydiSeaSe Table 56. These findings suggest that there is a spectrum of responsiveness to intravenous iron that extends to patients with serum ferritin levels as high as 1200 ng/mL. Concerns have been raised about the potential toxicity of intravenous iron supplements, including cellular and vascular damage from oxidative stress and impaired white blood cell function based on in vitro studies. However, observational studies have not demonstrated increased hospitalizations or mortality in patients undergoing hemodialysis receiving an average of less than 400 mg of intravenous iron per month, and intravenous iron therapy was not identified as a risk factor for bacteremia in patients undergoing hemodialysis in a multivariate analysis. Liver magnetic resonance imaging studies of patients undergoing hemodialysis have shown abnormally high iron content, which correlates with serum ferritin level and cumulative iron dose. Serial liver biopsies in patients with hemochromatosis showed no significant organ injury when the serum ferritin level was less than 2000 ng/ mL. Two new iron products have become available that provide lower doses of iron on a more continuous basis for patients undergoing dialysis and thereby may decrease the risk of excessive iron storage. This is manifested by prolonged bleeding time, abnormal studies of platelet aggregation and adhesiveness, and decreased release of platelet factor 3. Thrombocytopenia has been reported to rarely occur in patients undergoing hemodialysis with polysulfone membranes sterilized by electron beam technology. The clinical manifestations of these abnormalities include an increased tendency to and increased duration of bleeding after trauma and in the setting of serosal inflammation. This often manifests as epistaxis, bleeding with tooth brushing, and easy bruisability, but it can result in life-threatening gastrointestinal hemorrhage or hemorrhagic pericarditis. The bleeding diathesis is only partially corrected by dialysis, and larger molecules that accumulate in the setting of kidney failure, such as parathyroid hormone, have also been implicated. This is often associated with high levels of acute phase reactants such as serum ferritin, C-reactive protein, and erythrocyte sedimentation rate, but the source of the inflammation/infection may not be readily apparent. Transfusions are considered a last resort because of the potential development of sensitization affecting future transplantation candidacy and the small risk of blood-borne infections. There is no single Hb concentration that necessitates transfusion, and 524 Section10-chronicKidneydiSeaSe Conjugated estrogens (Premarin) act to reduce bleeding for up to 14 days, but the onset of action takes 6 hours. The mechanism of action may be related to inhibition of vascular nitric oxide production. The onset of action of cryoprecipitate is 1 hour, and its effect peaks at 12 hours. The response to cryoprecipitate is highly variable, and it should be reserved for life-threatening hemorrhage. The platelet hemostatic defect in uremia does not appear to protect against vascular access thrombosis, which is a common problem in patients on hemodialysis. The use of antiplatelet agents such as aspirin and clopidogrel to preserve vascular access may be associated with an unacceptably high rate of bleeding and is not recommended. When given in prophylactic doses, enoxaparin has not been shown to increase the risk of bleeding complications irrespective of the degree of impairment of kidney function. This may be responsible for the transient hypoxia that is sometimes observed during hemodialysis, and it is completely reversed by the end of the dialysis treatment. The function of granulocytes, including chemotaxis, adherence, phagocytosis, and production of reactive oxygen species, is altered in uremia; these changes may also be exacerbated by exposure to unmodified cellulosic membranes. Impaired granulocyte function is associated with increased susceptibility to infection with encapsulated bacteria, such as Staphylococcus, contributing to the high incidence of these infections in patients undergoing dialysis. Monocyte and lymphocyte function are also impaired in uremia, leading to a decrease in cellular-type immunity. This may manifest as an increased susceptibility to viral infections such as influenza, decreased response to vaccinations, and anergy to immunologic skin testing. The activity of autoimmune diseases such as systemic lupus erythematosus may be attenuated after uremia supervenes. An impairment of cytokine release decreases the febrile response to pathogens in uremic patients so that infections may go unnoticed and may become more serious before diagnosis. The clinical implication is that symptoms suggestive of infection must trigger an aggressive diagnostic and therapeutic response in this vulnerable population. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and erythropoietin. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. Ferric pyrophosphate citrate administered via dialysate reduces erythropoiesis-stimulating agent use and maintains hemoglobin in hemodialysis patients. Darbeopetin alfa impact on health status in diabetes patient with kidney disease: a randomized trial. Peritoneal dialysis and transplantation are covered in detail elsewhere in the Primer. It is important to note that the distribution of pore sizes for high-flux membranes is such that it does not allow for the passage of albumin. These fibers are encased in a plastic tubing device that allows blood to be pumped from the patient through the hollow fibers while an aqueous solution, the dialysate, is pumped outside the fibers, typically in the opposite direction of the blood flow (countercurrent), to maximize the diffusion gradients across the membranes and along the length of the dialyzer. The first are called "low-flux" membranes and are made up of fibers with small pore sizes, which allow the diffusion of small solutes such as urea and water but not the passage of larger molecules such as 2-microglobulin. Because of these larger pores, the rate of water transfer (ultrafiltration coefficient) is much higher than that for low-flux membranes. The manufacturing process of these membranes is such that, regardless of whether it is a low-flux or a high-flux Diffusion describes the movement of solutes from a milieu with high concentrations across a semipermeable membrane into a milieu where it is in lower concentration. The rate and amount of solute that diffuses across the membrane in either direction depend on the difference in concentration between the blood and dialysate compartments; the molecular size of the solute; the characteristics of the membrane including its surface area, thickness, and porosity; and the conditions of flow. These membrane characteristics are generally labeled mass transfer characteristic or coefficient of diffusion and are specific for the membrane used and the solute under consideration. Thus, as blood is pumped and traverses through the dialyzer inside hollow fibers, the urea concentration of the blood is reduced; concurrently, the urea concentration of the dialysate increases as it flows outside the hollow fibers in the opposite direction. If the blood and dialysate were to flow in the same direction, then the urea concentration gradient between the blood and dialysate compartments would be considerably reduced at the exit site of the dialyzer, whereas a countercurrent flow ensures a maximum difference in concentration along the entire dialyzer length and therefore higher flux of solute from the blood compartment into the dialysate compartment. The principles of diffusion apply not only to urea and other solutes that have a higher concentration in the blood than dialysate, but also to the diffusion of substances that have a higher concentration in the dialysate than blood. An example of the latter is the diffusion of bicarbonate from the dialysate into the blood compartment. The rate of diffusion (R) of a small blood solute like urea across the dialyzer membrane is proportional to the blood solute concentration (C) and is governed by laws of first-order kinetics. The curves are constructed based partially on data and partially on theoretical projection. The actual values may vary depending on the surface area of the membrane and operating conditions. The curve for native glomeruli represents the summation of all the glomeruli in two normal kidneys. Clearance of solutes by diffusion (via either conventional or high-efficiency/high-flux dialysis) deteriorates rapidly with increases in the molecular mass of the solute. In contrast, clearance by convection (hemofiltration or glomeruli) remains constant over a wide range of molecular mass. Because of their small pores, they also tend to have low ultrafiltration coefficients, although the ultrafiltration coefficient can be increased by increasing the surface area of the membrane. A low-flux membrane can be either high efficiency or low efficiency for urea transport, depending on its surface area and, to a lesser extent, its thickness. A high-flux membrane can be either high efficiency or low efficiency, depending on its surface area and, to a lesser extent, its thickness. It remains constant during intermittent treatments as both blood concentrations of small solutes (C) and solute removal rates (R) decrease simultaneously. The simple equation for solute clearance mentioned above does not take into account convective clearance of solutes. Convection refers to the mass transport of solutes along with the fluid it is dissolved in (plasma water) and is driven by the higher hydrostatic pressures in the blood compartment generated by the blood pump. The amount of solute removed by convection is not dependent on the concentration gradient of the solute, but rather on the difference in hydrostatic pressure between the blood and dialysate compartment and a specific membrane characteristic, termed the "sieving coefficient. The relative contribution of convective transport to overall clearance depends on the pore size of the membrane as well as the size and charge of the solute. In general, the relative contribution of convective transport to the overall clearance for small molecules, such as urea, is minor, but it is more substantial for larger molecules. Because this represents the net loss of solute (both diffusive and convective) and does not depend on the partitioning of the solute between plasma water and red blood cells or on calculation of the sieving coefficient of the membrane, it is a more accurate measurement of solute clearance. In this technique, there is no dialysate flow, and the ultrafiltrate has the same composition as plasma water. In convective removal techniques, the removal of small molecules is limited by their sieving coefficient "S" as well as the total volume of the ultrafiltrate. In contrast, diffusive removal is dependent on the concentration gradient and, therefore, is more efficient for the removal of small solutes. Because of the requirement of large volumes of sterile substitution solutions to replace the ultrafiltrate, these techniques are not widely used for the treatment of chronic dialysis patients in the United States. Because of diffusive loss across the semipermeable hemodialysis membrane (dotted line), the plasma concentration in the blood outlet is much lower. The thin arrow across the dialysis membrane represents a small amount of fluid loss (which is not necessary for solute removal). A high dialysate flow rate is used to maintain the concentration gradient across the dialysis membrane for solute removal. Plasma concentrations of solutes in the blood compartment remain unchanged as blood travels the length of the fiber and are similar to their concentrations in the ultrafiltrate. The hemofiltration membrane (broken line) has relatively large pores, which allow the necessary removal of a large volume of fluid (heavy arrow). Replacement fluid is infused into the blood outlet to lower the plasma concentration of solutes and compensate for the fluid loss. Analogous to hemofiltration, plasma concentration of solutes remains unchanged throughout the length of the glomerular capillary and is similar to that in Bowman space. Fluid removal across the glomerular basement membrane (broken curve) is large (heavy arrow). Reabsorption of fluid from the renal tubules lowers the plasma concentration of the solutes. This plateau is reached at different clearance values depending on the size of the solute and the specific membrane characteristics (porosity, thickness, surface charge, the chemical composition of the membrane, etc. These summative membrane characteristics are called the mass transfer coefficient (Ko). The mass transfer coefficient is specific for the membrane used and the solute being considered; for dialyzers, this is usually represented as KoA, where A is the effective surface area of the specific dialyzer. Manufacturers generally provide the KoA of the different solutes for the specific dialyzer, and the clearance of specific solutes at different blood and dialysate concentrations can be calculated from such values. Thus if the maximum blood flow rate (above which the negative arterial pressure prepump exceeds -250 mm Hg) is 350 mL/min, then the optimal dialysate flow rate is around 600 to 700 mL/min. The mass transfer coefficient is usually represented as KoA, where A is the effective surface area of the specific dialyzer. The total amount of solute removed during a dialysis procedure can be calculated from Kt (where K, the clearance in mL/min, is multiplied by the time [t] of the procedure in minutes); this assumes that the clearance (K) remains constant throughout the time of the procedure. Thus the dose of dialysis is usually defined as Kt/V, where V is the volume of distribution of that particular solute. Urea has been the index molecule used to define the dose of dialysis as it is easily measured, is small and therefore diffuses readily across a dialysis membrane, and, importantly, its volume of distribution (total body water) can be calculated from the weight of the patient. Thus the dose of dialysis traditionally is defined in terms of urea, rather than other solutes, and the K in the earlier equation typically refers to urea clearance. Another important feature in the relationship between higher clearance and higher blood flow rate is the fact that, in the clinical setting, blood flow rate measured by the blood pump may not accurately represent the actual blood flow rate flowing through the hollow fibers of the dialyzer. Thus the use of higher blood flow rates can only improve clearance up to a certain point. This, in turn, leads to a higher risk of red blood cell lysis, presumably from the sudden change between the negative pressures in the blood tubing before the blood pump and the rapid rise in hydrostatic pressures after the pump. Finally, there are practical limits to increasing the dialysate flow rate; not only is there cost associated with preparing water for dialysate preparation, but, because of the limitation of where Cpost is the urea concentration at the completion of dialysis, and Cpre is the urea concentration before the start of dialysis. SoluteClearanceOtherThanUrea Although solute clearance by diffusion is dependent on the size of the solute molecule, other considerations, such as the electrical charge of the molecule and its effective size, also affect the net transfer of uremic solutes across the membrane. Although phosphate has a low molecular weight and, based on its molecular size, would be expected to be easily cleared by high-flux dialysis membranes, in reality, phosphate is cleared rather poorly during dialysis because of its highly negative charge and the large number of water molecules that circulate with it; in addition, because of the large intracellular reservoirs of phosphate and slow transfer from the intracellular to the plasma compartment, net phosphate clearance by dialysis is poor. Modern dialysis equipment adjusts these hydrostatic pressure gradients by varying the negative ("suction") pressure in the dialysate compartment rather than increasing the pressure in the blood compartment; this avoids the potential for increased lysis of red blood cells. However, because this rapid transfer of plasma water occurs at the inlet of the dialyzer, the concentration of protein (oncotic pressure) rapidly rises in the blood compartment; because these proteins are also negatively charged, there is a corresponding development of a "concentration polarization" due to a rapid increase in negatively charged plasma protein concentration at the membrane surface (inside the blood compartment).
Unusual presentations anxiety 4 months postpartum generic venlor 75 mg line, such as necrosis of the tongue and of the penis anxiety youtube 75 mg venlor order visa, as well as visceral involvement of the lungs anxiety symptoms even on medication venlor 75 mg purchase overnight delivery, pancreas anxiety service dog order genuine venlor online, and intestines anxiety from alcohol purchase generic venlor pills, have been described. Examination may not only show a violaceous rash, skin nodules, skin firmness, and eschars, but also livedo reticularis and painful hyperesthesia of the skin. Nonhealing ulcerations of the skin and gangrene resistant to medical therapy often lead to amputation, uncontrollable sepsis, and death. Histologically, there is extensive medial calcification of small arteries, arterioles, capillaries, and venules, as well as intimal proliferation, endovascular fibrosis, and sometimes thrombosis. Anecdotal reports suggest that sodium thiosulfate, bisphosphonate therapy, daily hemodialysis, hyperbaric oxygen treatment, vitamin K, and normalization of serum phosphate levels may improve outcomes. This protein is normally released into the plasma with cell turnover and cleared by the kidney. Clinical manifestations of dialysis-related amyloidosis include destructive arthropathy, bone cysts, carpal tunnel syndrome, and fractures. Kidney transplant, high-flux hemodialysis, or hemofiltration, all of which provide increased clearance of 2M, may be beneficial (see Chapter 57). Some studies suggest that better control of serum phosphate, as well as use of noncalcium compared with calcium-based phosphate binders to control hyperphosphatemia, may be associated with improved outcomes. It may have hypocalcemic effects in vivo, and it has been shown to inhibit osteoclastic bone resorption in vitro. They use a capture antibody that binds near the N-terminus and a second solid phase-coupled antibody that binds to the C-terminus. Bone histomorphometric analysis of the biopsy specimen includes assessment of bone and fibrosis volumes, amount of osteoid and mineralization, and number of osteoblasts and osteoclasts seen on bony surfaces. The long-term impact of this more conservative management strategy still remains to be determined. Other biochemical markers of bone turnover are being developed that may provide a more accurate assessment of osteoblast and osteoclast activity in bone. Efforts to correlate the different subtypes of bone disease with various markers of bone remodeling in both dialysis and predialysis patients are areas of ongoing research. Furthermore, prospective studies are required to determine whether evaluating trends in biomarker concentrations could guide therapeutic decisions. Osteoclast-mediated bone resorption of secondary hyperparathyroidism results in cortical thinning and the classic radiographic evidence of subperiosteal, intracortical, and endosteal bone resorption. Subperiosteal erosions are best seen at the distal ends of the phalanges and clavicles and at the sacroiliac joints. Radiographically, expansile lytic lesions (brown tumors) can be seen in severe osteitis fibrosis. Pseudofractures, which appear as wide, radiolucent bands perpendicular to the bone long axis, can be seen in osteomalacia. These recommendations are influenced by data linking an elevated serum phosphorus concentration or an elevated calcium concentration to increased mortality and by the growing concern that excessive calcium exposure may increase the risk of cardiovascular calcification. Nonetheless, these guidelines are a first step toward standardizing the approach to this difficult disorder. The various tools for treating hyperphosphatemia and secondary hyperparathyroidism include dietary phosphorus restriction, calcium-based and noncalcium-based phosphate binders, calcitriol or other active vitamin D analogues, calcimimetics, daily or nocturnal hemodialysis, and parathyroidectomy. There are actually three major sources of exogenous phosphorus to be considered: natural phosphate (as cellular and protein constituents) contained in raw or unprocessed foods, phosphate added to foods during processing (daily exposure may be as high as 1000 mg), and phosphate in dietary supplements/medications. Dairy products, nuts, beer, and chocolate all have a high content of phosphorus (see Chapter 53). For patients who are undergoing thrice-weekly dialysis and are receiving adequate nutrition, dietary phosphate restriction will be inadequate to correct the positive phosphate balance, especially in the presence of concurrent active vitamin D therapy, which increases phosphorus absorption from the gut. More frequent and prolonged hemodialysis (see Chapter 57) has been associated with lower serum phosphorus levels, but with thrice-weekly hemodialysis, phosphate binders are almost invariably required. For many years, calcium-based phosphate binders were the mainstay of therapy to control serum phosphate levels. Commonly used calcium-based phosphate binders include calcium carbonate and calcium acetate. Calcium carbonate contains 500 mg of elemental calcium in a 1250-mg tablet (40%), whereas calcium acetate contains 169 mg of elemental calcium in one 667-mg tablet (25%). Calcium-based phosphate binders should be taken with meals to maximize binding of ingested phosphorus in the gut. When they are taken in the fasting state, more calcium is absorbed systemically and less phosphorus is bound. The concomitant use of active vitamin D sterols increases calcium absorption and the risk of hypercalcemia. Calcium acetate has greater phosphorus-binding capacity than calcium carbonate, potentially allowing the use of lower doses of calcium binder. However, various small trials have not shown significant differences in the prevalence of hypercalcemia between these two compounds. This, taken with growing concern about the possible clinical consequences of vascular calcifications, has led to the greater use of noncalcium binders. Sevelamer is a noncalcium phosphate binder containing cross-linked polyallylamine hydrochloride. It acts as an ion exchange polymer to bind phosphorus in the gut but is less effective than calcium on a weight basis. However, in human trials, sevelamer, when titrated to meet serum phosphorus goals, appeared equal in efficacy to the calcium-containing binders. Sevelamer has been associated with fewer arterial calcifications than calcium-based phosphate binders in dialysis patients. Sevelamer is more costly than calcium binders and may be associated with gastrointestinal side effects at higher doses that can limit its use in some individuals. Prospective trials comparing the effect of sevelamer versus calcium-containing phosphate binders on mortality produced equivocal results. One small, randomized trial with 127 incident hemodialysis patients monitored for a mean of 44 months demonstrated a significant overall survival advantage for sevelamer, although specific cardiovascular mortality was not assessed. In addition, patients who remained in the study for longer than 2 years on treatment with sevelamer had a decrease in all-cause mortality. The short duration of follow-up, the high dropout rate, and the fact that the study was not powered statistically to detect differences in specific causes of death are limitations of this study. This study suffers, however, from a moderate risk of bias and therefore should be interpreted with caution. Although they are the most effective binders, aluminumcontaining phosphate binders are not often used because of the potential for systemic aluminum absorption and subsequent neurologic, hematologic, and bone toxicity. Absorption of aluminum is increased by the concomitant 502 Section10-chronicKidneydiSeaSe use of sodium citrate for metabolic acidosis. Because of the potential for long-term toxicity, aluminum-containing antacids should be used only for a short period (<4 weeks) and only for severe hyperphosphatemia that is refractory to other treatments. Lanthanum, like aluminum, is a trivalent cation with an ability to chelate dietary phosphate, but it has low systemic absorption. Mild gastrointestinal symptoms were the most common side effect in the lanthanum group. Lanthanum, unlike sevelamer, is an effective binder even in the acidic environment of the gut and does not bind bile acids. Adherence may be better than with calcium-based binders or sevelamer as a result of a lower pill burden. Because there is accumulation of small amounts of lanthanum over time, safety concerns have been raised. Sucroferric oxyhydroxide and ferric citrate have recently become available on the market. The added value of these iron-based phosphate binders as compared with established phosphate binders remains to be demonstrated. The individual choice should be guided by considerations about concomitant therapies and the present calcium and phosphate levels. There is no uniform agreement about the route, dose, and type of active vitamin D analogue that should be given. Some of the available vitamin D analogues may cause less hypercalcemia than calcitriol, possibly because of decreased intestinal effect on calcium absorption. When paricalcitol was compared with calcitriol in a large observational study of hemodialysis patients, its use was associated with significantly lower mortality. Although this study initially raised questions about the extent to which efforts to control secondary hyperparathyroidism with vitamin D analogues might cause harm, subsequent retrospective studies suggested improved survival in dialysis patients treated with active vitamin D analogues compared with patients who did not receive vitamin D at all. However, a recent analysis of a large international dialysis database supported the possibility that the effect of vitamin D may represent a patient selection bias. Prospective clinical trials are needed to determine whether vitamin D therapy offers a survival advantage in dialysis patients. Of note, in Europe, the oral route has been the preferential route of administration for years. In fact, there is usually a reduction in serum calcium and a tendency toward reduced serum phosphorus with calcimimetics. Additional studies are needed to evaluate the effect of cinacalcet in altering the natural history of parathyroid gland hyperplasia. Either a subtotal parathyroidectomy or a total parathyroidectomy with forearm gland implantation can be performed. Some surgeons favor the latter procedure to avoid the need for repeated invasive neck surgery if hyperparathyroidism recurs. Both subtotal and total parathyroidectomy with implantation are effective methods, and there are no studies comparing these approaches. Nonetheless, there is a 15% to 30% recurrence rate of hyperparathyroidism after complete or partial parathyroidectomy. Percutaneous ethanol injection into the gland as an ablation procedure for hyperparathyroidism refractory to medical management is performed in some centers in lieu of surgical parathyroidectomy. If severe or symptomatic hypocalcemia develops, treatment with a continuous calcium infusion is necessary. Concomitant treatment with oral calcitriol before and after parathyroidectomy may mitigate the hungry bone syndrome. Metabolic acidosis causes an efflux of calcium from bone as bone buffers hydrogen ions with carbonate release. Chronic metabolic acidosis should be corrected with sodium bicarbonate supplementation. The demonstration of a significantly increased risk of hypercalcemia in patients treated with paricalcitol compared with placebo, in the absence of beneficial effects calcimimetics in combination with active vitamin analogues, however, did not reduce vascular calcifications. However, the results of secondary analyses suggest that cinacalcet may yet be beneficial in this population or a subset. Intermediate or hard endpoint clinical trials with entelcalcetide are currently lacking. In kidney transplant recipients, bisphosphonate may protect against immunosuppressioninduced bone loss and prevent fracture. It is not uncommon for patients to develop hypophosphatemia after kidney transplantation. More aggressive use of phosphate supplementation may exacerbate secondary hyperparathyroidism. Transplantation also prevents, but does not reverse, bone damage from amyloidosis caused by 2M deposition. Symptoms of amyloidosis frequently abate after transplantation, perhaps because of concomitant steroid therapy. Although successful kidney transplantation corrects many of the conditions that lead to disordered mineral metabolism associated with kidney failure, the glucocorticoids used to prevent rejection result in increased bone fragility, osteoporosis, and increased fracture rates. Other risk factors for fractures in this population include the presence of pretransplantation fracture, diabetes mellitus, and older age. In fact, the risk of fractures is greater in kidney transplant recipients than in patients on dialysis, at least in the first years after transplantation. Steroid minimization most probably accounts to a large extent for this favorable trend. Calcium and vitamin D supplementation may be effective in counteracting the effects of glucocorticoids to reduce gastrointestinal calcium absorption. However, given the concern for antiresorptive treatment-induced adynamic bone disease in this population and the lack of data on reduced facture incidence with this approach, there are currently no consensus recommendations on the use of this therapy in kidney recipients. It most typically occurs in the femoral heads or other weight-bearing joints and is characterized by the collapse of surface bone and cartilage. The pathogenesis of this disorder is not clear, but it is probably related to prednisone therapy. Magnetic resonance imaging is the most sensitive technique to evaluate patients with hip pain after transplantation for the presence of avascular necrosis. A multicenter study on the effects of lanthanum carbonate (Fosrenol) and calcium carbonate on renal bone disease in dialysis patients. Fibroblastic growth factor 23 and mortality among patients undergoing hemodialysis. Renal osteodystrophy in the first decade of the new millennium: analysis of 630 bone biopsies in black and white patients. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Effect of etelcalcetide vs cinacalcet on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism: a randomized clinical trial. Sevelamer attenuates the progression of coronary and aortic calcification in hemodialysis patients.
Order venlor us. Doyle talks About His Social Anxiety More Misfits Shows and Gene Simmons interview.
References
- Lewis AB, Freed MD, Heymann MA, et al. Side effects of therapy with prostaglandin E1 in infants with critical congenital heart disease. Circulation 1981;64:893-98.
- Pearn J. Neuromuscular paralysis caused by tick envenomation. J Neurol Sci. 1977;34:37-42.
- Stannard JP, Bucknell AL: Rupture of the triceps tendon associated with steroid injections. Am J Sports Med 21:482, 1993.
- Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol 2006; 7:392-401.
- Hartman KL, Liang BA. Exceptions to informed consent in emergency medicine. Hosp Physician. 1999;1999:53-59.
- Lucchetti V, Capasso F, Caputo M, et al. Intracoronary shunt prevents left ventricular function impairment during beating heart coronary revascularization. Eur J Cardiothorac Surg 1999; 15:255-259.
- Anzueto A, Baughman RP, Guntupalli KK, et al. Aerosolized surfactant in adults with sepsis-induced acute respiratory distress syndrome. Exosurf Acute Respiratory Distress Syndrome Sepsis Study Group. N Engl J Med 1996;334:1417-21.