
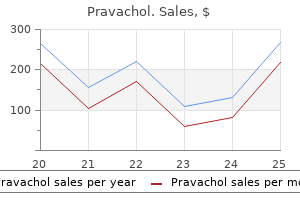
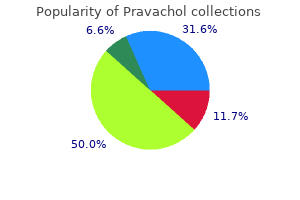
Pravachol
| Contato
Página Inicial
Adrianne K. Thompson, MD
- Chief, Body Imaging
- Wilford Hall Medical Center
- Lackland AFB, Texas
Ask the patient if she is pregnant or a diabetic cholesterol medication no grapefruit 20 mg pravachol order fast delivery, both of which place the patient at risk for vaginitis ldl cholesterol levels chart australia order pravachol 10mg on-line. Take a sexual history to determine the number of partners cholesterol medication problems pravachol 20mg low cost, the frequency of intercourse cholesterol shrimp or scallops order pravachol online from canada, the types of sexual practices cholesterol lowering foods chart pravachol 10 mg buy on line, and the type of birth control that was used. Note that sexual history taking is sensitive and should be done by an experienced practitioner with great sensitivity. The most common symptom is a vaginal discharge, which may be frothy, thick, or malodorous. The patient is likely to have external swelling of the vulva, internal inflammation, pain, and itching. Vaginal examination should take place under the following conditions: not during menses, no douching or vaginal sprays for 24 hours prior to examination, and no sexual intercourse without a condom for 24 hours prior to the examination. Physical examination generally reveals some type of discharge, such as frothy, malodorous, greenish-yellow, purulent vaginal discharge (trichomoniasis); thick, cottage cheese like discharge (candidiasis); or malodorous, thin, grayish-white, foul, fishy odor discharge (bacterial). The external and internal genitalia are often reddened, inflamed, and painful on examination. Women with candidiasis often have patches on their vaginal walls and cervix and signs of inflammation. Women with trichomoniasis have a strawberry spot on the vaginal surface and cervix. Provide a private environment to allow the patient to answer questions without being embarrassed. Diagnostic Highlights Test Saline wet mount (wet prep) Normal Result Negative for organism (not visualized under microscope) Negative for fungus/ bacteria Abnormality With Condition Positive for organism (visualized under microscope); clue cells seen for bacterial vaginosis Positive for fungus/ bacteria; fishy, amine odor present for bacteria Candida: pH 4. Patients are told to stop using any douches and feminine hygiene sprays, to observe good nutrition, and to maintain healthy exercise patterns. Many women with candidiasis use over-the-counter treatment, which may or may not be effective. Encourage the patient to use appropriate hygiene techniques by wiping from front to back after urinating or defecating. Teach the patient to avoid wearing tight-fitting clothing (pantyhose, tight pants or jeans) and to wear cotton underwear rather than synthetics. Explain to patients that the risk of getting vaginal infections increases if one has sex with more than one person. Teach the patient to abstain from sexual intercourse until the infection is resolved. The pain and itching from vaginitis may be quite intense until the medication is effective. Some women find that by applying wet compresses and then using a hair dryer on a cool setting several times a day provides some relief of itching. For yeast infections, tepid sodium bicarbonate baths and applying cornstarch to dry the area may increase comfort during treatment. Be informed about which sexually transmitted diseases need to be reported to the local health department. It is caused by low estrogen levels and results in vaginal dryness, itching, dyspareunia, urinary frequency, and increased urinary tract infections. Varicose Veins 1143 · Low-dose vaginal estrogen therapy is the treatment of choice. It is effective and safe for most women, except for women with hormone-sensitive cancers. Newer treatment options include selective estrogen receptor modulators, vaginal dehydroepiandrosterone, and laser therapy. Nonprescription treatments include vaginal lubricants, moisturizers, and dilators. Make sure the patient understands all aspects of the treatment regimen with particular attention to taking the full course of medication therapy. They occur most often in the lower extremities but can appear anywhere in the body. Primary varicosities are caused by incompetent valves in the superficial saphenous veins, whereas secondary varicosities are the result of impaired blood flow in the deep veins. Primary varicosities tend to occur in both legs, whereas secondary varicosities usually occur in only one leg. Normally, in a ladderlike fashion, perforator veins connect the deep vein and the superficial vein systems, promoting drainage of the lower extremities. The underlying problem of varicose veins is reverse venous flow, which is also known as venous insufficiency syndrome. The blood that is circulated by retrograde flow has already been circulated once, is poorly oxygenated, and contains lactate. It does not provide body tissues with helpful nutrients, and it contributes to congestion. Fluid accumulates in the extremity, causing swelling, inflammatory dermatitis, and skin breakdown. Other complications include infection, cellulitis, discoloration, ulceration, thrombophlebitis, and loss of limbs. Primary varicose veins occur because of incompetent venous valves that result in venous 1144 Varicose Veins hypertension. Some people have an inherited tendency for elevated superficial venous pressures, and others have weakness of vein walls in the absence of elevated venous pressure. Several behavioral and environmental factors cause increased venous pressure and venous stasis that result in dilation and stretching of the vessel wall. Increased venous pressure results from being erect, which shifts the full weight of the venous column of blood to the legs. Prolonged standing increases venous pressure because leg muscle use is less; therefore, blood return to the heart is decreased. Secondary varicose veins result from deep venous thrombosis and its sequelae or congenital anatomical abnormalities. Heavy lifting, genetic factors, obesity, thrombophlebitis, pregnancy, trauma, abdominal tumors, congenital or acquired arteriovenous fistulae, trauma to the legs, and congenital venous malformations are among the risk factors for varicose veins. Chronic liver diseases such as cirrhosis can cause varicosities in the rectum, abdomen, and esophagus. Prevalence increases with age, peaking in the 50s and 60s and decreasing dramatically after age 70. Varicose veins are more common in women; in the population over age 30, four times as many women as men are affected. The prevalence of venous disease and varicose veins is higher in developed than in developing nations, likely due to alterations in lifestyle, nutrition, body mass index, and physical activity. Elicit a history of symptoms, paying particular attention to pain and discomfort, changes in appearance of vessels and skin, and complaints of a sensation of fullness or tingling of the lower extremities. Determine if the patient has experienced any bleeding from the varicose veins, as well as leg edema, exercise intolerance, tenderness along the course of the vein, pruritus, burning sensations, or cramping. Take an occupational history with particular attention to those jobs that require long hours of walking or standing. Question the patient about lifetime weight changes, such as changes during pregnancy and sustained periods of being overweight. Ask the patient if there is a personal or family history of heart disease, obesity, thrombophlebitis, or varicose veins. Superficial veins can be inspected for distension and prominence as well as accompanying symptoms such as ulceration, swelling, blanching, and a sense of fullness of the legs. The number, severity, and type of varicosities determine the symptoms experienced by the individual. With the patient standing, examine the legs from the groin to the foot in good lighting. Time of examination is a factor because secondary varicosities are more symptomatic earlier in the day. Varicose Veins 1145 Patients may complain of heaviness, aching, edema, muscle cramps, increased fatigue of lower leg muscles, and itching. Determine if the patient has discoloration, ulcerations, translucent or shiny skin, and swelling of the legs. Severity of discomfort may be difficult to assess and is unrelated to the size of the varicosity. The patient with varicose veins has usually been dealing with a progressively worsening condition. Assess the patient for any problems with body image because of the changed appearance of skin surface that is caused by varicose veins. Question the patient to determine possible lifestyle adjustments to decrease symptoms. Diagnostic Highlights General Comments: Incompetency of the deep and superficial veins can be diagnosed by several tests. Treatment for varicose veins is aimed at improving blood flow, reducing retrograde flow, reducing injury, and reducing venous pressure. To give support and promote venous return, physicians recommend wearing elastic stockings. If the varicosities are moderately severe, the physician may recommend antiembolism stockings or elastic bandages or, in severe cases, custom-fitted heavy-weight stockings with graduated pressure. Experts also recommend that the patient stop smoking to prevent vasoconstriction of the vessels. A nonsurgical treatment is the use of sclerotherapy for varicose and spider veins to prevent retrograde blood flow. Sclerotherapy is palliative, not curative, and is often done for cosmetic reasons after surgical intervention. A sclerosing agent, such as sodium tetradecyl sulfate (Sotradecol) or polidocanol, is injected into the vein, followed by a compression bandage for a period of time. The expert application of this therapy is important because some of the underlying problems may be in deeper, subsurface veins. Newer techniques, such as radiofrequency ablation and endovenous laser therapy, are also available with expert consultation. A surgical approach to varicose veins is vein ligation (tying off) or stripping (removal) of the incompetent veins. Removal of the vein is performed through multiple short incisions from the ankle to the groin. A compression dressing is applied after surgery and is maintained for 3 to 5 days. Elevate the foot of the bed 6 to 9 inches to keep the leg above the heart when the postoperative client is in bed. Pharmacologic Highlights No medications are generally used to treat varicose veins, except for analgesics following surgery. Independent Nursing interventions are aimed at educating the patient to decrease venous stasis, promote venous return, and prevent tissue injury. To prevent vein distention by compression of superficial veins, teach the patient to apply elastic support stockings before standing and to avoid long periods of standing. The patient should be encouraged to engage in an exercise program of walking to strengthen leg muscles. Teach the patient to avoid crossing the legs when sitting and to elevate the legs when sitting or lying down. The patient should be taught to observe the skin when removing stockings to check for signs of irritation, edema, decreased nerve sensation, and discoloration. For patients who have had sclerotherapy, teaching should focus on activity restrictions. Teach the patient to wait 24 to 48 hours after the procedure before showering and to avoid tub baths. Prepare the patient by advising him or her to expect ecchymosis and some scarring, which will fade in several weeks. Caution the patient that some residual brown staining may remain at the injection sites. Acute effects of graduated elastic compression stockings in patients with symptomatic varicose veins: A randomized double blind placebo controlled trial. To prevent worsening of varicosities, teach the patient to avoid prolonged standing in one place, to avoid sitting with the legs crossed, to elevate the legs frequently during the day, to wear support stockings as ordered, and to drink 2 to 3 L of fluid daily. Teach the patient the purpose, dosage, route, and side effects of any medications ordered. Teach the patient to recognize and observe daily for signs of thrombophlebitis, which include redness, local swelling, warmth, discoloration (not related to surgery area), and back pain on bending. Teach the patient to report any signs of infection, such as redness at incision sites or injection sites, severe pain, purulent drainage, fever, or swelling. A dysrhythmia can be the result of a disturbance in the ability of the myocardial cell to conduct an impulse (conductivity), a disturbance in the ability to initiate and maintain an inherent rhythm spontaneously (automaticity), or a combination of both. Risk factors include coronary heart disease, use of recreational drugs such as cocaine, electrolyte abnormalities, family history of rhythm disorders, and toxicities from medications such as digitalis, procainamide, epinephrine, aminophylline, tricyclic antidepressants, beta-adrenergic stimulants, or quinidine. In addition, many of the medications that aging people take to manage heart failure (digitalis and diuretics in particular) place them at risk for drug toxicities and electrolyte imbalances. If the patient is unable to provide a history of the life-threatening event, obtain it from a witness. Many patients with suspected cardiac dysrhythmias describe a history of symptoms indicating periods of decreased cardiac output. They may report dizziness, syncope, dyspnea, palpitations, diaphoresis, chest pain, and activity intolerance.
Both can appear as elevated peripheral lesions; however cholesterol in foods guide buy cheap pravachol 10mg on line, the following characteristics can help differentiate the 2 (Table 40-1) cholesterol test for diabetes buy pravachol paypal. Response to Scleral Depression Scleral depression tends to partially flatten a retinal detachment cholesterol ratio ldl hdl calculator purchase 20mg pravachol with mastercard, as the subretinal fluid is pushed through the retinal break into the vitreous cavity cholesterol test calculator pravachol 20mg order overnight delivery, whereas a schisis is unlikely to flatten with depression because the fluid tends to be trapped within the schisis cavity cholesterol levels as you age discount pravachol 10 mg mastercard. Visual Field Testing A schisis will produce an absolute visual field defect because the connections between the inner and outer retina have been severed. Patients with a detachment will be able to appreciate the T-shaped shadow (T-sign), whereas patients with a schisis will not, as their scotoma is absolute. However, it should be noted that some authors question the utility of this test, noting that retinal whitening can sometimes be achieved in areas with overlying detached retina, especially if the laser power is turned high enough. Prevalence and long-term natural course of retinoschisis among elderly individuals: the Copenhagen City Eye Study. The long-term natural history of senile retinoschisis with implications for management. Indirect ophthalmoscope perimetry in patients with retinal detachment or retinoschisis. Differentiation of degenerative retinoschisis from retinal detachment using optical coherence tomography. Marfan syndrome, Ehlers-Danlos syndrome, and homocystinuria are all hereditary systemic connective tissue disorders which influence collagen cross-linking causing thin and collapsible sclera. The result is sclera that is less elastic and prone to stretching, resulting in axial myopia and crystalline lens subluxation. Intraocular surgery to remove the dislocated crystalline lens secondarily increases the risk of retinal detachment and is associated with a higher incidence of vitreous loss. Predisposing retinal lesions, such as lattice degeneration, is common in these systemic diseases. Aggressive treatment of retinal breaks and prophylactic laser retinopexy treatment of lattice degeneration are advised. When these vessels regress, the contracting force creates excess traction on the ischemic and atrophic retina resulting in retinal breaks. Fifty percent of patients with necrotizing herpetic retinitis develop retinal detachments that frequently have multiple, large, or posterior retinal breaks and may also involve proliferative vitreoretinopathy. This external manipulation creates repetitive anterior-posterior vitreous traction. Close surveillance with a dilated fundus examination with scleral depression for patients with acquired systemic conditions that predispose to retinal detachments is recommended. Prompt referral to a vitreoretinal specialist is necessary in the event of a newly diagnosed retinal break or retinal detachment. Long-term surgical outcomes of retinal detachment in patients with Stickler Syndrome. Incidence of retinal detachment associated with atopic dermatitis in Japan: a review of cases from 1992 to 2011. Peripheral vitreoretinal traction often occurs in the setting of posterior vitreous detachment. Retinal breaks are more likely to occur in areas of particularly adherent vitreous and/or retinal weakness. Preoperative retinopexy with laser photocoagulation or cryotherapy should be applied to all symptomatic retinal breaks and all horseshoe retinal tears whether symptomatic or not. Asymptomatic operculated holes and atrophic holes do not necessarily require treatment, but the option of treatment should be discussed with the patient. Prophylactic cryotherapy or laser cerclage (360° photocoagulation placed posterior to the vitreous base) is recommended in patients with genetic proof or high clinical suspicion of Fekrat S, ed. Given the strong association (up to 70%) of peripheral retinal breaks in nondiabetic eyes with vitreous hemorrhage, these eyes must be examined especially carefully. Ultrasonography should be employed in cases in which complete visualization of the retinal periphery is precluded by media opacity. If removal of the hemorrhage is required for adequate fundus visualization to facilitate retinal treatment, then vitrectomy should be performed either prior to cataract surgery or, in cases of dense cataract, concomitant with or immediately following cataract surgery. You should ask all patients if they were born early (< 32 weeks of gestational age) or if they were told that they were born with a low birth weight. Thus, treatment directed at retinal conditions that are associated with traction or inflammation should be helpful in reducing the chance of postoperative macular edema. Retinal or systemic conditions that signal a high risk for postoperative macular edema include: Disorders of the vitreomacular interface (vitreomacular adhesion, posterior hyaloidal contraction, epiretinal membrane). In such cases, it is advisable to remove the cataract first, allow complete recovery, and then reassess the extent of macula-related vision impairment. The incidence of macular edema following even uneventful cataract surgery is higher in a diabetic eye, even in the absence of diabetic retinopathy, than in nondiabetic eyes. While the conventional teaching has been to control diabetic retinopathy and eradicate macular edema (traditionally using laser photocoagulation) completely for several months prior to cataract surgery, this may not always be achievable, and the time required to do so may delay the time to vision improvement. In such cases of silent retinopathy or featureless retina, chronic retinal ischemia has damaged the native retinal vasculature so severely that the typical compensatory microaneurymal and neovascular changes cannot arise. When unrecognized and untreated, these eyes can progress rapidly to neovascular glaucoma within a short time following cataract surgery. As in diabetic retinopathy, retinal ischemia arising from venous occlusion can lead to visionthreatening macular edema or vitreous hemorrhage due to posterior segment neovascularization. In eyes with vitreous hemorrhage due to neovascularization, preoperative peripheral scatter retinal laser photocoagulation to the affected area is recommended. Pharmacokinetic and clinical data suggest that these peak levels occur, and therapeutic effect begins, at 3 to 7 days following intravitreal injection. Typically, symptoms of inflammation develop within several days following intravitreal injection. Though these complications are uncommon, it may be preferable to pass safely through this risk period before performing cataract surgery. Prevention of retinal detachment in Stickler syndrome: the Cambridge prophylactic cryotherapy protocol. Risk factors and incidence of macular edema after cataract surgery: a database study of 81984 eyes. Prophylactic non-steroidal anti-inflammatory drugs for the prevention of macular oedema after cataract surgery. Pseudophakic cystoid macular edema prevention and risk factors; prospective study with adjunctive once daily topical nepafenac 0. First, while there are many points to consider in the patient history, perhaps the most important is the presence or absence of symptoms. In many fields of medicine, patients with the same clinical problem, one symptomatic and the other asymptomatic, may be treated quite differently; for example, in the settings of cholelithiasis where the presence of symptoms may indicate intervention that otherwise may have been deferred. While self-evident, it is worth recognizing that in the absence of current or past symptoms, it is not possible to make a patient symptomatically better. In the setting of an individual without the expected capacity to recognize or report symptoms, however, this factor is less important and possibly irrelevant. Other anatomic factors to consider include macula status, presence of a retinal dialysis, and lens status. Fundus photograph of the left eye of a 59-year-old female showing chronic, temporal retinal detachment associated with atrophic retinal holes and pigmentary changes. The patient has remained asymptomatic, with stable best-corrected visual acuity (20/20) and stable borders of the retinal detachment over 5 years of follow-up. Excellent outcomes may be obtained with retinal reattachment surgery using 3 distinct approaches: scleral buckling, pars plana vitrectomy, and/or pneumatic retinopexy. Patients need to be aware of this possibility, understand the risks and benefits of both observation and intervention, and agree to the management plan. While well-meaning, surgical intervention aimed at retinal reattachment can have untoward effects including cataract acceleration, glaucoma, infection, bleeding, cystoid macular edema, diplopia, refractive shift, and the development of proliferative vitreoretinopathy, which can ultimately lead to a poorer visual outcome. If serial observation is agreed upon, we review steps for monocular self-monitoring of the visual field with the patient and develop a management plan if progression is noted. Finally, specific ocular characteristics may increase the likelihood of intervention including extensive location, high myopia, superior and bullous characteristics, and absence of a demarcation line. Therefore, specific patient education related to any additional risk factors must be considered and management decisions should be individualized. Spontaneous regression and disappearance of subclinical rhegmatogenous retinal detachment. Round atrophic holes in lattice degeneration-an important cause of phakic retinal detachment. Spectral domain optical coherence tomography imaging of subretinal bands associated with chronic retinal detachments. Posterior vitreous detachment after cataract extraction in non-myopic eyes and the resulting retinal lesions. Demarcation laser photocoagulation of selected macula-sparing rhegmatogenous retinal detachments. If the patient is asymptomatic and/or visual acuity is 20/40 or better, observation may be indicated with periodic re-evaluation for a drop in visual acuity or the onset of symptoms. It can persist with a stable level of retinal disruption or it may progress Fekrat S, ed. This recombinant protease achieves vitreomacular release through its proteolytic activity against laminin and fibronectin-2 key components of the vitreoretinal interface. In most cases, these adverse events have been temporary and a good visual outcome was ultimately obtained, but there have been select reports of permanent scotoma and visual loss. It is hypothesized that the buoyant force induced by the gas bubble causes a mechanical separation of the vitreoretinal interface. The procedure was initially described in the early 1990s as an alternative to vitrectomy to close macular holes. Ocriplasmin and pneumatic vitreolysis remain options; however, one must be prepared for vitrectomy if these less invasive options are not successful. Further clinical studies are needed to characterize eyes that will respond to pneumatic vitreolysis. To maximize gains in visual acuity, it is likely best not to wait to more than several months before intervention. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. Treatment of vitreomacular traction with intravitreal perfluoropropane (C3F8) injection. Even among compliant patients with frequent ophthalmic exams and timely scatter panretinal laser photocoagulation, vitrectomy still becomes necessary in at least 5% of patients. The 2 predominant classic indications for diabetic vitrectomy, nonclearing vitreous hemorrhage and tractional retinal detachment involving the macula, have remained the same since the results of the Diabetic Retinopathy Vitrectomy Study were published in the 1980s. We have divided indications for diabetic vitrectomy into 5 broad categories (Table 45-1). These categories include (A) retinal detachment, (B) hemorrhage, (C) severe retinal neovascularization, (D) macular pathology, and (E) postvitrectomy. As it is not uncommon for eyes to have more than one indication for diabetic vitrectomy, a sixth category was added to include F. This usually occurs when retinal neovascularization develops along the vascular arcades with multiple epicenters, becomes fibrotic, and contracts causing the underlying retina to elevate and detach. Tractional retinal detachment not involving the macula is not an indication for surgery because it can remain stable. This is especially true when the retinal neovascular component is inactive and fibrotic, most often seen after full prior-panretinal laser photocoagulation has been performed. These detachments can progress very quickly and require extensive hyaloid and membrane removal on a mobile retina to repair. Many breaks are only identified intraoperatively because fibrosis and hemorrhage may prevent preoperative visualization. Their management is similar in eyes without retinopathy with particular attention to postoperative worsening of retinopathy and macular edema. Hemorrhage Vitreous hemorrhage is the other classic indication for diabetic vitrectomy, especially when it is visually significant and nonclearing. The hemorrhage is considered visually significant if it is responsible for a vision of less than 20/400 and the opacity prevents laser photocoagulation. To determine if the hemorrhage is nonclearing, the patient would have to give a history of no improvement or be examined without improvement for at least 3 to 4 weeks. Dense premacular hemorrhage can lead to progressive fibrosis and, even if it clears, can result in a premacular fibrotic membrane. Subretinal hemorrhage is rare and generally associated with a very adherent and attached hyaloid or retinal break. Other vitreous opacities, when severe enough to prevent diagnosis and treatment of diabetic retinopathy, are a potential indication for vitrectomy. The natural history of this process is fibrosis and traction as the neovascularization cicatrizes and results in a broad-based tractional retinal detachment with a tabletop configuration. The tractional detachments can sometimes encircle the macula before the center detaches. The prognosis for vision is inversely proportional to the extent of active retinal neovascularization. Vitrectomy in these cases can be difficult and when successful can prevent inevitable blindness. Vitreomacular traction syndrome complicating diabetic retinopathy imaged by optical coherence tomography. Macular Pathology In a small subset of eyes, a taut hyaloid results in persistent macular edema due to tangential vitreous traction. The macular edema is usually diffuse and removing the hyaloid is very effective in decreasing the edema. Premacular fibrosis with or without neovascularization can occur and in some cases, consists of a fibrotic and contracted hyaloid membrane in front of the macula causing obscuration of the fovea.
Autoantibodies have been reported in association with administration of isoniazid cholesterol test recommendations order 10 mg pravachol visa, penicillin cholesterol lowering foods benecol purchase 10 mg pravachol mastercard, and phenytoin cholesterol lowering diet plan uk buy cheapest pravachol and pravachol. Familial Combined Factor Deficiencies Multiple combined coagulation factor deficiencies have been described (Table 4 fasting cholesterol test vitamins order pravachol 10mg mastercard. Familial combined deficiencies may be due to a single genetic defect that results in multiple factor deficiencies or to different genetic defects that lead to each deficient factor cholesterol medication uk pravachol 20mg low price. These patients usually have bleeding symptoms after trauma and during or after surgery. In patients with the combined disorder, mild factor V deficiency is sometimes undiagnosed. Homozygous individuals can have spontaneous bleeding including epistaxis, easy bruising, gum bleeding, hemarthrosis, and menorrhagia. For major surgery, it may be necessary to raise factor V to near-normal levels through plasma exchange. The combined deficiency of the vitamin Kdependent factors was first described by McMillan and Roberts in 1966. These genes have already been characterized and identified in at least four individuals. Bleeding in individuals with combined deficiency of the vitamin Kdependent factors can on occasions be severe. Bleeding symptoms range from mild to severe and usually involves the skin and mucosae. Umbilical stump bleeding and intracerebral hemorrhage may occur when factor levels are extremely low. In some patients with a congenital deficiency of vitamin Kdependent clotting factors, the use of high doses of oral vitamin K may be beneficial. Hemorrhagic disease of the newborn may resemble the congenital deficiency syndrome that was once common. However, in recent times, most gravid women, as well as their newborns, are given prophylactic vitamin K, so this condition is now rare. When present, it can be easily treated with vitamin K, and symptoms do not return. Malabsorption can also cause vitamin K deficiency in children, but again, symptoms of malabsorption are evident, and the clotting defect is rapidly corrected by administration of vitamin K. Liver disease may lead to a decrease in vitamin Kdependent factors, and this cause can be suspected on the basis of abnormal liver function test results. Care must be taken to exclude the possibility of accidental or furtive ingestion of warfarin or superwarfarin, either of which may cause a deficiency of the same factors as those seen in a congenital deficiency syndrome. Special consideration must be given to the class of coumarins now referred to as superwarfarins. These were developed to overcome the resistance of rats to warfarin-containing rodenticides. In contrast to warfarin, superwarfarins have an extremely long half-life and, when ingested, are stored in the liver and have a high affinity for lipids. After being ingested by humans, they may remain in the body for months, and the resulting bleeding disorder can closely resemble the congenital deficiency syndrome unless one takes a careful history and determines that the bleeding symptoms were acquired. Poisoning with superwarfarin may result from accidental administration (most commonly seen in children), psychiatric conditions, industrial exposure, surreptitious ingestion, or deliberate self-poisoning with denial (Munchausen syndrome). Cases of surreptitious ingestion of superwarfarin may be encountered in medical or paramedical personnel who take the compound for secondary gain; for example, a spouse may ingest the substance to punish or gain sympathy from the partner. The potency of superwarfarin is 100 times that of warfarin, and the half-life is between 16 and 69 days, compared with 37 hours for warfarin. Superwarfarins block the carboxylation of vitamin Kdependent factors by inhibiting the vitamin K 2,3-epoxide reductase enzyme in the liver. Bleeding is the most common manifestation and may occur from any mucosal site, soft tissue, or organ. Decreased levels of vitamin Kdependent factors are the hallmark of this condition. Special assays are needed to detect the presence of warfarin or superwarfarin in blood. Assays for brodifacoum and other superwarfarins are not usually readily available in most clinical laboratories; thus samples must be sent to special centers for clinical and forensic confirmation. The latter can be given orally or parenterally at a daily maintenance dose that may range from 20 mg to more than 100 mg, depending on the severity of the hemorrhagic diathesis. It is important to remember that because of the long halflife of the substance and its affinity for lipids, vitamin K must be given over a long period, sometimes for several months to a year. When bleeding occurs, plasma or specific factor concentrates may be used for treatment. Since its discovery, more than 10 families have been identified who have this disorder. Pathogenesis and Genetics Individuals with 2-plasmin inhibitor deficiency exhibit a hemorrhagic tendency caused by reduced inhibition of plasmin, accompanied by resultant increased fibrinolytic activity. Deficiency is inherited in an autosomal recessive pattern, with no predilection for sex or race. The gene is located on chromosome 17, and a variety of genetic defects, including additions, small deletions, and specific nucleotide substitutions, have been reported. Clinical Manifestations Bleeding manifestations are more pronounced in homozygous individuals and are characterized by easy bruising, epistaxis, hematuria, menorrhagia, and hemarthrosis. Heterozygous individuals usually have hemorrhagic symptoms only in association with trauma. Differential Diagnosis Deficiency of 2-plasmin inhibitor may also be acquired and has been reported in individuals with liver failure, amyloidosis, solid tumor, acute promyelocytic leukemia, and disseminated intravascular coagulation. During bleeding situations, -aminocaproic acid may be used orally or intravenously at a dosage of 2 to 3 g every 6 hours. She also had excessive bleeding after a tooth extraction, removal of an ingrown toenail, and hemorrhagic ovarian cysts. Bleeding manifestations occurred after trauma, which induced an increase in the level of the mutant enzyme, which is an acute phase reactant. This substitution essentially converts 1-antitrypsin into a protein having both antithrombin and antifactor Xa activity. One individual had severe bleeding episodes with soft tissue hematoma, hematuria, and melena. In the second and third individuals, low protein C activity (13% and 0% of normal, respectively) was also seen, but its cause and role are not clear. The consultant should be aware that mild prolongation of results on any of the screening tests of coagulation should be investigated. If such abnormalities appear to have been lifelong, the patient most likely has a congenital bleeding disorder. However, it should be emphasized that the most important diagnostic information to be sought regarding a hereditary bleeding disease is a personal or family history of bleeding spontaneously or after trauma or surgery. Some mildly affected patients may have no bleeding until late in life, and the consultant will have to carefully assess the family history to rule out acquired causes of a hemorrhagic disorder. Because many diseases are recessive in inheritance, a high degree of consideration must be given to consanguinity. Finally, the consultant should remember the importance of genetic counseling for affected patients and their families. Potential adverse effects of therapy, including possible allergic reactions and any specific adverse effects associated with therapeutic products, should always be explained to the patient. When an unusual diagnosis is made in a family member, consideration should be given to notifying and possibly testing other members of the family. Cost should not be the deciding factor in treatment but should always be considered. For example, recombinant products, although they often are more expensive than plasma-derived clotting factor concentrates, are preferred because they are less likely to be contaminated with potentially transmissible agents that are not susceptible to currently used eradication techniques. Although he will be missed, his impact on hemostasis and thrombosis will live within us forever. Molecular mechanisms accounting for fibrinogen deficiency: from large deletions to intracellular retention of misfolded proteins. Laboratory and genetic investigation of mutations accounting for congenital fibrinogen disorders. Spontaneous intracranial bleeding in two patients with congenital afibrinogenaemia and the role of replacement therapy. Successful treatment of two brothers with congenital afibrinogenemia for splenic rupture using heat-and-solvent detergent-treated fibrinogen concentrate. Bone cysts in patients with afibrinogenaemia: a literature review and two new cases. Platelet aggregation occurs in congenital afibrinogenemia despite the absence of fibrinogen or its fragments in plasma and platelets, as demonstrated by immunoenzymology. Delayed-type hypersensitivity skin reactions in congenital afibrinogenemia lack fibrin deposition and induration. High incidence of valproate-induced coagulation disorders in children receiving valproic acid: a prospective study. Changes in antithrombin and fibrinogen levels during induction chemotherapy with L-asparaginase in adult patients with acute lymphoblastic leukemia or lymphoblastic lymphoma. Precipitating antifibrinogen antibody appears after fibrinogen infusions in a patient with congenital afibrinogenemia. Congenital afibrinogenemia: vascular changes and multiple thromboses induced by fibrinogen infusions and contraceptive medication. Successive bleeding and thrombotic complications in a patient with afibrinogenemia: a case report. Dysfibrinogenemia: from molecular anomalies to clinical manifestations and management. Clinical phenotype, laboratory features and genotype of 35 patients with heritable dysfibrinogenaemia. Rational, high quality laboratory monitoring before, during, and after infusion of prothrombin complex concentrates. Proteolysis of plasma-derived factor V following its endocytosis by megakaryocytes forms the platelet-derived factor V/Va pool. Factor V is complexed with multimerin in resting platelet lysates and colocalizes multimerin in platelet alpha-granules. Residual platelet factor V ensures thrombin generation in patients with severe congenital factor V deficiency and mild bleeding symptoms. Platelets and platelet-derived factor Va confer hemostatic competence in complete factor V deficiency. Rescue of fatal neonatal hemorrhage in factor V deficient mice by low level transgene expression. Abnormal sialic acid content of the dysfibrinogenemia associated with liver disease. Incomplete embryonic lethality and fatal neonatal hemorrhage caused by prothrombin deficiency in mice. Lupus anticoagulant-hypothrombinemia syndrome: report of two cases and review of the literature. A new method for characterization and epitope determination of a lupus anticoagulantassociated neutralizing antiprothrombin antibody. Blood coagulation factor X deficiency causes partial embryonic lethality and fatal neonatal bleeding in mice. Coagulation factor activity and clinical bleeding severity in rare bleeding disorders: results from the European Network of Rare Bleeding Disorders. Successful treatment of transient acquired factor X deficiency by plasmapheresis with concomitant intravenous immunoglobulin and steroid therapy. Lupus anticoagulant associated with transient severe factor X deficiency: a report of two patients presenting with major bleeding complications. Novel factor X deficiency: normal partial thromboplastin time and associated spindle cell thymoma. Antibody-induced acute factor X deficiency: clinical manifestations and properties of the antibody. The contact activation and kallikrein/kinin systems: pathophysiologic and physiologic activities. A familial hemorrhagic trait associated with a deficiency of a clot-promoting fraction of plasma. A case of IgM antibodies which inhibit the contact activation of blood coagulation. IgM inhibitors of the contact activation phase of coagulation in chlorpromazine-treated patients. Efficacy, safety and pharmacokinetics of a new high-purity factor X concentrate in subjects with hereditary factor X deficiency. Experience of a new high-purity factor X concentrate in subjects with hereditary factor X deficiency undergoing surgery. Presurgical plasma exchange is ineffective in correcting amyloid associated factor X deficiency. Utility of factor X concentrate for the treatment of acquired factor X deficiency in systemic light-chain amyloidosis. New hemophilia-like disease caused by deficiency of a third plasma thromboplastin factor. Thrombotic events in patients with congenital prekallikrein deficiency: a critical evaluation of all reported cases. A hitherto undescribed congenital haemorrhagic diathesis probably due to fibrin stabilizing factor deficiency. Guidelines on the laboratory aspects of assays used in haemostasis and thrombosis.
Investigators found that transverse lie and other malpresentations were more common in pregnancies complicated by placenta previa cholesterol norms buy generic pravachol 20 mg on line. Cesarean deliveries and blood transfusions were more common in pregnancies diagnosed with placenta previa cholesterol disease order pravachol 10 mg with amex. Gestational age at delivery was lower cholesterol triglycerides chart order pravachol 10mg otc, and neonates were less likely to weigh over 4 cholesterol medication and muscle pain 10 mg pravachol order visa,000 grams at birth what cholesterol medication has the least side effects generic pravachol 10 mg otc. The authors concluded that the neonatal prognosis in placenta previa is primarily influenced by neonate gestational age, not by the previa. Pregnant patients diagnosed with placenta previa and delivered at term do not appear to have an elevated the risk for perinatal mortality and morbidity. The causitive organism, originally named Pneumocystis carinii, has been renamed P. While it is classified as a fungal infection, it does not respond to antifungal therapy. Epidemiological surveys have found that by age 3 to 4, most humans have been exposed to the pathogen. Early in the infection, the organisms line up along the alveolar wall near the type I pneumocytes. The alveoli become infiltrated with a fluid that contains proteins, organisms in varying states of development, cellular debris, and surfactant. As the disease progresses, alveoli hypertrophy, type I pneumocytes die, and the patient has markedly diminished gas exchange. Other vulnerable populations include patients who receive corticosteroid therapy and organ transplantation. Organisms in this family are often found in the lungs of healthy people, and airborne exposure in healthy children occurs globally. Risk factors include any condition that causes immunodeficiency, such as cancer. They often report weight loss and fatigue on exertion and become short of breath even when speaking. Ask about a recent history of anorexia, nausea, vomiting, weight loss, or a low-grade intermittent fever. Common symptoms include fever, dyspnea on exertion, nonproductive cough, stridor, nasal flaring, and chest tightness. Check for pallor, flushing, cyanosis, and signs of hypoxemia such as mental status changes and agitation. Auscultate the lungs for abnormal breath sounds, crackles, or diminished or absent breath sounds, either unilaterally or bilaterally. The patient may experience anxiety, depression, or difficulty in coping with the change in health status. Some patients may require intubation and mechanical ventilation to maintain gas exchange. If the patient is not intubated and is able to take oral nutrition, a high-calorie, protein-rich diet is recommended. If the patient cannot tolerate large amounts of food, smaller, more frequent meals can be offered. Oral narcotics may be given to reduce the respiratory rate and control anxiety, thereby improving comfort and gas exchange. Position the patient so that he or she is comfortable and breathes with as little effort as possible. Schedule diagnostic tests and patient care activities with ample rest periods between them. As the patient gains strength, encourage coughing and deep-breathing exercises and teach him or her how to perform incentive spirometry. Teach the patient guided imaging or relaxation techniques for nonpharmacologic relief of discomfort. Include the family and significant others in all teaching activities as appropriate. Risk factors included old age, female sex, longer time from onset to diagnosis, respiratory failure, and solid tumors. Teach the patient appropriate preventive measures, such as covering the mouth and nose while coughing when in contact with susceptible individuals. Teach the patient to recognize symptoms, such as dyspnea, chest pain, fatigue, weight loss, fever and chills, and productive cough, that should be reported to healthcare personnel. Pneumonia is an inflammatory condition of the interstitial lung tissue in which fluid and blood cells escape into the alveoli. More than 3 million people in the United States are diagnosed each year with pneumonia. As the organism multiplies, the alveolar spaces fill with fluid, white blood cells, and cellular debris from phagocytosis of the infectious agent. The infection spreads from the alveolus and can involve the distal airways (bronchopneumonia), part of a lobe (lobular pneumonia), or an entire lung (lobar pneumonia). The inflammatory process causes the lung tissue to stiffen, resulting in a decrease in lung compliance and an increase in the work of breathing. The fluid-filled alveoli cause a physiological shunt, meaning that venous blood passes unventilated portions of lung tissue and returns to the left atrium unoxygenated. As the arterial oxygen tension falls, the patient begins to exhibit the signs and symptoms of hypoxemia. In addition to hypoxemia, pneumonia can lead to complications such as Pneumonia 917 respiratory failure, lung abscess, and septic shock. Infection may spread via the bloodstream and cause endocarditis, pericarditis, meningitis, or bacteremia. Viral pneumonia occurs when a virus attacks bronchiolar epithelial cells and causes interstitial inflammation and desquamation, which eventually spread to the alveoli. Secondary pneumonia ensues from lung damage that was caused by the spread of bacteria from an infection elsewhere in the body or by a noxious chemical. Factors associated with aspiration pneumonia include old age, impaired gag reflex, surgical procedures, debilitating disease, and decreased level of consciousness. Organisms that cause typical pneumonia include Streptococcus pneumoniae (pneumococcus) and the Haemophilus and Staphylococcus species. Organisms that cause atypical pneumonia include the Legionella, Mycoplasma, and Chlamydia species. Risk factors for the development of pneumonia include cigarette smoking, chronic obstructive pulmonary disease, asthma, immunosuppression, protein pump inhibitors, alcohol abuse, major surgery, drug dependence or abuse, altered mental status, seizure disorder, and recent pulmonary infections with the flu or cold. Neonates with multisystem disease are also at risk for viral pneumonia caused by cytomegalovirus. More than 60% of hospitalizations and 85% of deaths from viral pneumonia occur in older adults. People over age 40 are at greater risk to contract all forms of bacterial pneumonia, with older men more susceptible to streptococcal bacterial pneumonia and Klebsiella bacterial pneumonia. While patterns exist with some populations, there are no definitive racial or ethnic considerations of clinical significance. Serious pneumonia in children and overall deaths from pneumonia for all ages occur more often in developing than in developed nations. The patient may have a history of a recent upper respiratory infection, influenza, or a viral syndrome. The patient may report a productive cough, fever, chest pain, or difficulty breathing. Establish any history of exposure to noxious gases, aspiration, or immunosuppressive therapy. Ask the patient to describe the type of cough and the nature of the sputum production. The major symptoms of pneumonia are cough, fever, sputum production, chest pain, and shortness of breath. Assess vital signs for rapid, weak, thready pulse; fever; and blood pressure changes such as hypotension and orthostasis (postural hypotension). The patient with pneumonia may be anxious, fatigued, and in pain from the constant coughing. The patient and family will likely be very anxious because of difficulty breathing and distressed over purulent sputum. Pneumonia can be life threatening if not treated promptly, and the family and patient will likely recognize this serious situation. Physicians may request regular measurements of peak and trough levels, especially for patients who are receiving aminoglycosides, which can produce severe side effects such as renal failure and hearing loss. Percussion and postural drainage may be prescribed to assist the patient in expectorating secretions. Pharmacologic Highlights Medication or Drug Class Antibiotics Dosage Varies with drug Description Depends on bacteria. Initial antibiotic: Macrolides including erythromycin, azithromycin, roxithromycin and clarithromycin. Other antibiotics: Penicillin G for streptococcal pneumonia; nafcillin or oxacillin for staphylococcal pneumonia; aminoglycoside or a cephalosporin for Klebsiella pneumonia; penicillin G or clindamycin for aspiration pneumonia. Encourage drinking 3 L of fluid daily, unless contraindicated, to help expectorate secretions. If the patient cannot cough up secretions, you may have to perform nasotracheal or orotracheal suction to maintain an open airway. Turn and position patients on bedrest to help keep the airway open and free of secretions. Elevate the head of the bed to at least 45 degrees to help the patient maintain an open airway and find positions that ease breathing. Place the patient in an upright position with both arms well supported on pillows or position the patient to lean forward and rest her or his arms on the overbed table. Involve the patient in as much decision making as possible and, when possible, include the family in teaching situations. Teach the importance of adequate rest and the deep-breathing and coughing exercises that are designed to clear lung secretions. Teach proper ways to dispose of secretions and proper hand-washing techniques to minimize the risk of spreading infection. Advise annual influenza vaccinations or avoidance of using antibiotics indiscriminately because such use creates a risk for upper airway colonization by antibiotic-resistant bacteria. The etiology and impact of co-infections in children hospitalized with communityacquired pneumonia. Children with co-infections had worse outcomes: longer lengths of stay, more need for mechanical ventilation, and more pulmonary effusions. The patient and family or significant others need to understand the importance of avoiding fatigue by limiting activity and taking frequent rests. Fluid intake should be maintained at approximately 3,000 mL/day so that the secretions remain thin. Teach the patient to maintain pulmonary hygiene measures of coughing, deep breathing, and incentive spirometry at home. Normally, the pleural space is a "potential space," a space that occurs between two adjacent structures that are normally pressed together. The area between the visceral and parietal pleura has a negative atmospheric pressure, creating a vacuum as well as containing a small amount of protective fluid to lubricate the tissues. In pneumothorax, air accumulates in the pleural space, and the pressure rises, leading to atelectasis (collapsed lung) and ineffective gas exchange. Spontaneous pneumothorax is not life threatening and occurs when a portion of the lung collapses without a known cause. Most experts suspect that it is due to the formation of small sacs of air that rupture, causing air to leak into the pleural space. Traumatic pneumothorax can be further classified as either open (when atmospheric air enters the pleural space) or closed (when air enters the pleural space from the lung). Traumatic pneumothoraces are most often associated with an injury resulting in a wound or puncture, disrupting the pleural space by changing the vacuum into a positive-pressure space. In open traumatic pneumothorax, a chest wall defect creates an opening that connects the outside atmospheric air to the pleural space. A gunshot or stab wound that leaves a hole in the chest wall is one cause of an open pneumothorax. The degree of distress and compromise that the patient experiences depends on the degree of collapse on the affected side. If air accumulation is not stopped, the entire mediastinum shifts toward the unaffected side, causing bilateral lung collapse, which is a life-threatening condition. Tension pneumothorax is a lifethreatening complication that can lead to shock, low blood pressure, and cardiopulmonary arrest. Blunt chest trauma and penetrating chest trauma are the primary causes of traumatic and tension pneumothorax. Other possible causes include therapeutic procedures such as thoracotomy, thoracentesis, and insertion of a central line. Risk factors for spontaneous pneumothorax include smoking; a tall, thin stature; Marfan syndrome; pregnancy; and family history. Spontaneous primary pneumothorax occurs most often in tall, thin men between ages 20 and 30. Traumatic injuries are more common in adolescent and young adult males than in other populations. Traditional Chinese medicine with acupuncture may lead to pneumothorax, which is the most serious complication reported in the literature, with an incidence of 1 in 5,000 individuals after acupuncture in the area of the lungs. Question if the patient has had shortness of breath, difficulty breathing, or fatigue.
Influence of thrombophilia on risk of recurrent venous thromboembolism while on warfarin: results from a randomized trial bad cholesterol levels nz order pravachol 20 mg with visa. The long-term recurrence risk of patients with unprovoked venous thromboembolism: an observational cohort study cholesterol in eggs 2012 pravachol 20mg purchase free shipping. Risk of recurrence after venous thromboembolism in men and women: patient level meta-analysis high cholesterol foods to eat list buy cheap pravachol. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study cholesterol deep conditioner pravachol 10mg buy cheap. Risk assessment of recurrence in patients with unprovoked deep vein thrombosis orpulmonary embolism: the Vienna prediction model cholesterol levels nz heart foundation purchase pravachol 10 mg on line. Epidemiology of first and recurrent venous thromboembolism: A population-based cohort study in patients without active cancer. Age at first venous thromboembolism and risk of recurrence: a prospective cohort study. Sex difference in the risk of recurrent venous thrombosis: A detailed analysis in four European cohorts. Survival and recurrent venous thromboembolism in patients with first proximal or isolated distal deep vein thrombosis and no pulmonary embolism. Does the clinical presentation and extent of venous thrombosis predict likelihood and type of recurrence Recurrent venous thromboembolism after deep vein thrombosis: incidence and risk factors. Patients with a first symptomatic unprovoked deep vein thrombosis are at higher 10. Long-term vs short-term therapy with vitamin K antagonists for symptomatic venous thromboembolism. Effectiveness and safety of novel oral anticoagulants as compared with vitamin K antagonists in the treatment of acute symptomatic venous thromboembolism: a systematic review and meta-analysis. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. D-dimer testing to select patients with a first unprovoked venous thromboembolism who can stop anticoagulant therapy. Systematicreview: D-dimer to predict recurrent disease after stopping anticoagulant therapy for unprovoked venous thromboembolism. Performance of five different bleeding-prediction scores in patients with acute pulmonary embolism. Predictive variables for major bleeding events in patients presenting with documented acute venous thromboembolism. Comparativevalidation of a novel risk score for predicting bleeding risk in anticoagulated patients With atrial fibrillation. Familial risk of venous thromboembolism in first-, second- and third-degree relatives: a nationwide family study in Sweden. The genetic basis of complex traits: rare variants or common gene, common disease. Taller height as a risk factor for venous thromboembolism: a Mendelian randomization meta-analysis. The epidemiology of pulmonary embolism: racial contrasts in incidence and in-hospital case fatality. Racial and regional differences in venous thromboembolism in the United States in 3 cohorts. Incidence of idiopathic deep venous thrombosis and secondary thromboembolism among ethnic groups in California. Factors that predict risk of thrombosis in relatives of patients with unprovoked venous thromboembolism. Factors that predict thrombosis in relatives of patients with venous thromboembolism. Consumer awareness and attitudes about insurance discrimination post enactment of the Genetic Information Nondiscrimination Act. The incidence of venous thromboembolism among Factor V Leiden carriers: a community-based cohort study. Presenting quantitative information about decision outcomes: a risk communication primer for patient decision aid developers. Hereditary risk factors of thrombophilia and probability of venous thromboembolism during pregnancy and the puerperium. Different combined oral contraceptives and the risk of venous thrombosis: systematic review and network meta-analysis. Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. Screening for factor V Leiden mutation before prescribing combination oral contraceptives. Investigation of relation between use of oral contraceptives and thromboembolic disease. Venous thrombosis in users of non-oral hormonal contraception: follow-up study, Denmark 2001-10. Risk of venous thromboembolism from use of oral contraceptives containing different progestogens and oestrogen doses: Danish cohort study, 2001-9. Risk of venous thrombosis: obesity and its joint effect with oral contraceptive use and prothrombotic mutations. Effect of tamoxifen on venous thromboembolic events in a breast cancer prevention trial. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Guidance for the evaluation and treatment of hereditary and acquired thrombophilia. A prospective cohort study on the absolute risks of venous thromboembolism and predictive value of screening asymptomatic relatives of patients with hereditary deficiencies of protein S, protein C or antithrombin. A riskbenefit analysis of factor V Leiden testing to improve pregnancy outcomes: a case study of the capabilities of decision modeling in genomics. Points to consider: Ethical, legal, and psychosocial implications of genetic testing in children and adolescents. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. Venous thromboembolism in childhood: A prospective two-year registry in the Netherlands. The incidence of venous thromboembolism in thrombophilic children: a prospective cohort study. The risk of mortality and the factor V Leiden mutation in a population-based cohort. Mortality and causes of death in families with the factor V Leiden mutation (resistance to activated protein C). The kinetics of hemostatic enzyme-antithrombin interactions in the presence of low molecular weight heparin. Coagulation and fibrinolysis in primary biliary cirrhosis compared with other liver disease and during orthotopic liver transplantation. Plasmaantithrombin levels correlate with albumin and total protein in gestational hypertension and preeclampsia. Clinical presentation and molecular basis of congenital antithrombin deficiency in children: a cohort study. Prevalence of antithrombin deficiency in healthy blood donors: A cross-sectional study. The clinical presentation and genotype of protein C deficiency with double mutations of the protein C gene. Characterization of a protein C activator from Agkistrodon contortrix contortrix venom. Multilaboratory testing in thrombophilia through the United Kingdom National External Quality Assessment Scheme (Blood Coagulation) Quality Assurance Program. Further evidence that activated protein C resistance affects protein C coagulant activity assays. Cerebral haemorrhagic infarction in young patients with hereditary protein C deficiency: evidence for spontaneous cerebral venous thrombosis. Factor V Leiden mutation, prothrombin gene mutation, and deficiencies in coagulation inhibitors associated with Budd-Chiari syndrome and portal vein thrombosis: results of a case-control study. Antithrombin, protein C and protein S levels in 127 consecutive young adults with ischemic stroke. Adult-onset arterial thrombosis in a pedigree of homozygous and heterozygous protein C deficiency. Anticoagulation therapy for thromboembolism prevention: a case of warfarin-induced skin necrosis in the setting of protein C deficiency. Recurrent venous thromboembolism in patients with a partial deficiency of protein S. Protein S testing in patients with protein S deficiency, factor V Leiden, and rivaroxaban by North American Specialized Coagulation Laboratories. Altered reference ranges for protein C and protein S during early pregnancy: Implications for the diagnosis of protein C and protein S deficiency during pregnancy. Changes in the plasma levels of vitamin K-dependent proteins C and S and of C4b-binding protein during pregnancy and oral contraception. Protein C and protein S levels can be accurately determined within 24 hours of diagnosis of acute venous thromboembolism. Normal levels of protein C and protein S tested in the acute phase of a venous thromboembolic event are not falsely elevated. Evidence of normal thrombin generation in cirrhosis despite abnormal conventional coagulation tests. Use of protein-C concentrate, heparin, and haemodiafiltration in meningococcus-induced purpura fulminans. Thromboembolic complications in the nephrotic syndrome: Pathophysiology and clinical management. Plasma concentrations of the natural anticoagulants protein C and protein S in patients with proteinuria. Different risks of thrombosis in four coagulation defects associated with inherited thrombophilia: a study of 150 families. Clinical relevance of decreased free protein S levels: results from a retrospective family cohort study involving 1143 relatives. Protein S activity during oral anticoagulation, in liver disease, and in disseminated intravascular coagulation. Activation and complexation of protein C and cleavage and decrease of protein S in plasma of patients with intravascular coagulation. Low total protein S antigen but high protein S activity due to decreased C4b-binding protein in neonates. Brief report: autoimmune protein S deficiency in a boy with severe thromboembolic disease. Thrombophilia differences in splanchnic vein thrombosis and lower extremity deep venous thrombosis in North America. Interaction of hereditary thrombophilia and traditional cardiovascular risk factors on the risk of arterial thromboembolism: pooled analysis of four family cohort studies. Familial thrombophilia due to a previously unrecognized mechanism characterized by poor anticoagulant response to activated protein C: prediction of a cofactor to activated protein C. Linkage between inherited resistance to activated protein C and factor V gene mutation in venous thrombosis. Association of idiopathic venous thromboembolism with single point-mutation at Arg506 of factor V. Mutation in blood coagulation factor V associated with resistance to activated protein C. Factor V Cambridge: a new mutation (Arg306>Thr) associated with resistance to activated protein C. Factor V I359T: a novel mutation associated with thrombosis and resistance to activated protein C. Functional characterization of factor V-Ile359Thr: a novel mutation associated with thrombosis. Factor V Leiden and the risk for venous thromboembolism in the adult Danish population. Risk of venous thromboembolism associated with single and combined effects of Factor V Leiden, Prothrombin 20210A and Methylenetethraydrofolate reductase C677T: a meta-analysis involving over 11,000 cases and 21,000 controls. Risk of recurrent venous thrombosis in homozygous carriers and double heterozygous carriers of factor V Leiden and prothrombin G20210A. Do incident and recurrent venous thromboembolism risks truly differ between heterozygous and homozygous Factor V Leiden carriers Coagulation studies, factor V Leiden, and anticardiolipin antibodies in 40 cases of cerebral venous thrombosis. Factor V Leiden mutation is a risk factor for cerebral venous thrombosis: a case-control study of 55 patients. Associations of coagulation factor V Leiden and prothrombin G20210A mutations with BuddChiari syndrome and portal vein thrombosis: a systematic review and meta-analysis. Sevenhaemostaticgene polymorphisms in coronary disease: meta-analysis of 66,155 cases and 91,307 controls. Linkage analysis demonstrates that the prothrombin G20210A mutation jointly influences plasma prothrombin levels and risk of thrombosis. A single genetic origin for the common prothrombotic G20210A polymorphism in the prothrombin gene. Prevalence and geographical variation of prothrombin G20210A mutation in patients with cerebral vein thrombosis: A systematic review and meta-analysis. Anticardiolipin antibodies: detection by radioimmunoassay and association with thrombosis in systemic lupus erythematosus.
Cheap pravachol 10mg mastercard. Bad Cholesterol hdl and ldl in the blood stream medical animation.
References
- Patrick DL, Erickson P: Assessing health-related quality of life for clinical decision-making, Chapter 19. In Walker SR, Rosser RM, editors: Quality of life assessment: key issues in the 1990s, Dordrecht, Netherlands, 1993, Kluwer Academic Publishers. Patrick DL, Martin ML, Bushnell DM, et al: Cultural adaptation of a qualityof- life measure for urinary incontinence, Eur Urol 36(5):427-435, 1999.
- Dumusc A, So A. Interleukin- 1 as a therapeutic target in gout. Curr Opin Rheumatol 2015; 27(2):156-63.
- Shalabi MM, Gortemaker A, Van't Hof MA, et al. Implant surface roughness and bone healing: a systematic review. J Dent Res 2006;85:496-500.
- Beckman JA: Giant cell arteritis, Curr Treat Options Cardiovasc Med 2(3):213-218, 2000.