
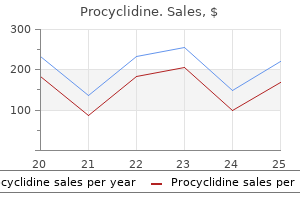
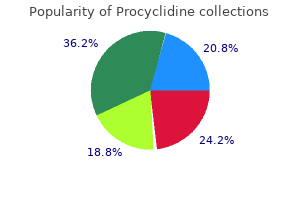
Procyclidine
| Contato
Página Inicial
Sovrin M. Shah, MD
- Assistant Professor of Urology,
- Albert Einstein College of Medicine, Bronx, New York
- Physician-in-Charge,
- Female Urology, Voiding Dysfunction, and Pelvic
- Reconstructive Surgery,
- Beth Israel Medical Center, New York, New York
Therefore symptoms congestive heart failure order procyclidine 5 mg without prescription, one can create pure magnification by calculating the front curvature and lens thickness medicine under tongue 5 mg procyclidine order fast delivery, and then adjusting the back curvature to render the lens afocal symptoms in spanish buy procyclidine without a prescription. In practice medicine zantac quality procyclidine 5 mg, however moroccanoil treatment procyclidine 5 mg otc, the magnification achieved by an iseikonic lens rarely exceeds 5%, which is insufficient to be of practical benefit in the correction of unilateral aphakia. Disconcerting curves are noted; they change their shape as the patient moves the eyes and looks through different zones of the lenses. Patients usually learn to adapt to this by restricting their gaze to the axial zone of their lenses and by moving their head rather then their eyes to look around. The prismatic effect of aphakic lenses produces a ring scotoma around the edge of the lens. Alternatively, a lenticular lens may be used, whereby the desired correction is limited to the central portion or aperture, but the surrounding margin of the lens acts as a carrier. In the early 1970s, Pearce reinstated the posterior chamber lens with his variation of the Binkhorst four-loop lens. With this gel, the diopter power can be adjusted by varying the quantity of gel injected into the capsular bag. If the eye is quiet and has good visual acuity preoperatively, however, it may be difficult to justify an operation, which always carries a risk of complications. Alternative methods for correcting aphakia include spectacles, contact lenses, keratomileusis, epikeratophakia, and keratophakia. With contact lenses, the patient can avoid the problems that arise with aphakic spectacles, such as image magnification or distortion. However, aphakic spectacle wearers have to contend with several problems caused by the high refractive power of the lenses required (about +10 D or higher). Object O will be visible to the spectacle-wearer through the periphery of the spectacle lens (c). As the eye rotates, moving from point a to point b, the ring scotoma moves in the opposite direction, from point A to point B (d). The surgeon removes the central epithelium with mechanical débridement and performs a peripheral lamellar dissection at the bottom of the trephine cut. As a result of the myriad complications experienced with the older designs of anterior chamber lenses, many ophthalmologists are still hesitant to use these types of lenses. Thus, anterior chamber lenses could play a useful role in secondary lens implantation. The surgeon must also be able to apply the cornea to the lathe and grind to achieve the precise correction. Several techniques and their potential advantages and untoward effects are highlighted later in this chapter. These lenses achieve their goal by refractive or diffractive optical principles to distribute light to different focal points and provide two or more planes of focus. The Restor lens uses a combination of three complementary technologies: apodization, diffraction and refraction. Its apodized diffractive optic design provides the ability to focus light correctly on the retina for images at various distances without mechanical movement of the lens. This technology optimally manages light energy delivered to the retina because it distributes the appropriate amount of light to near and distant focal points, regardless of the lighting situation. Apodized diffractive optics are designed to improve image quality while minimizing visual disturbances. The Rezoom multifocal lens is divided into five different zones with each zone designed for different light and focal distances. This lens has proportioned the size of its zones to provide for good vision in a range of light conditions. For instance, some zones have been designed to offer greater low light/distance vision support during night driving. For example, a decentration of 2 mm or more could cause a loss of near visual acuity; at the other extreme, pupillary apertures of less than 2 mm could cause a loss of distance visual acuity. Either loss could require corrective spectacles, thus defeating the purpose of the multifocal lens. The important requirements for an effective optic material include the following: (1) it must be material that can be turned on the lathe or molded and polished to a high optical quality; (2) it must be biocompatible and durable, with little induction of inflammation and fibrosis; (3) it should be nonantigenic and noncarcinogenic; (4) it must be sterilizable;6 and (5) it must maintain its optical clarity and not develop opacities or granulations. In the early 1980s, Biedner and Sachs implanted glass lenses in 10 eyes with good effect and no complications. One way of avoiding the problems associated with rigid lenses is to use softer polymeric materials for lenses. Mechanical disadvantages of foldable lenses include decentration and lens tilting, which may occur after capsular bag fixation with plate lens designs. There have been reports of grooves on soft lenses that correspond to the forceps used during implantation. Intraocular loops today are made of polypropylene (Prolene), a synthetic polymer first marketed in the late 1950s. First, polypropylene materials can attract circulating inflammatory cells by activation of complement. Polyamide can be heat-sterilized because it is able to withstand high temperatures as well as high-energy radiation. Polyamide is flexible and can be manufactured in many different shapes and sizes but is not stable in the eye. Nylon undergoes hydrolytic biodegradation in the eye; as time goes by, it implants into tissue. There have been many published reports of nylon loops and sutures breaking and degrading within the eye. It soon became clear, however, that the excessive weight and the cutting effect of the sharp metal edges in contact with uveal tissue caused many complications. The posterior chamber is bounded by: (1) the ciliary processes and the clefts between them, (2) the lens (resting in its capsular bag) and the lens suspensory ligament, and (3) the pigment epithelium of the iris. The posterior surgical limbus is defined as the location where the white of the sclera meets the blue-gray zone of the corneoscleral limbus. This region is relatively avascular and is located anterior to the retina (the scalloped, posterior margin of the pars plana fits into the edge of the ora serrata, which is the very beginning of the retina). The pars plana is, therefore, a safe point at which to traverse the sclera and choroid to enter the vitreous. Beginning with the external landmarks, the orbicularis oculi muscle is a flat muscle with many functions, including lowering the upper lid and raising the lower lid to squeeze the eyelids shut. An elliptic muscle, the orbicularis oculi, surrounds the orbital margin and extends onto the temporal region and cheek, into the eyelids, and behind the lacrimal sac. To prevent the eyelids from squeezing shut during surgery, temporary paralysis of the orbicularis muscle is achieved by paralysis of the temporal and zygomatic branches of the facial nerve, which supply the orbicularis oculi. In the past, seventh cranial nerve akinesia (by painful transcutaneous injection) and globe anesthesia were performed in two separate steps. In current practice, a combination of high volumes of local anesthetic and hyaluronidase is injected directly into the orbit. This one injection spreads from the orbit through the orbital septum, causing akinesia of the orbicularis oculi. When performing a retrobulbar block, one should not introduce the regional anesthesia needles into the posterior 1. Complications of retrobulbar nerve blocks include retrobulbar hemorrhage, retinal vascular occlusion, optic nerve trauma, and optic atrophy. A superior rectus suture is useful to maintain downward rotation of the globe, to retract a conjunctival flap from the limbus, and to help lift a deeply set globe from the orbit. Evaluation may include a complete eye examination, gonioscopy, keratometry, and A-scan biometry. With a high-magnification slit lamp, the eye can be examined to assess the health of the corneal endothelial cells. Any procedure on the eye can cause loss of endothelial cells, and if there is a critically low number of cells preoperatively, a secondary lens implantation could precipitate corneal decompensation. This complication can be minimized by performing temporal corneal incisions: it is thought that the temporal incision is safer because the cell count is typically lowest superiorly at the site of the original cataract incision. If the patient has a high cup-to-disk ratio with advanced visual field changes, the surgeon should carefully weigh the benefits versus the risks of secondary lens implantation. The surgeon can correct a distorted pupil by cutting any vitreous adhesions to the wound and can close a sector iridectomy with a 100 polypropylene or a 100 nylon suture. It is useful to dilate the pupil to diagnose adhesions between the iris and the capsule. Because the footplates of an anterior chamber lens rest in the recess of an open angle, areas of peripheral anterior synechiae should be noted and avoided as sites of implantation. Another key feature of the preoperative evaluation is the examination of the macula with biomicroscopy and indirect Secondary Intraocular Lens Implantation ophthalmoscopy. Secondary lens implantation is possible in eyes with permanent macular changes due to macular degeneration or residual macular edema. A-scan ultrasonography measures axial length, whereas keratometry determines corneal power and astigmatism. First, the echospikes represented correspond to the corneal and retinal interfaces; the anterior and posterior lens echospikes are absent. Second, when performing the preoperative ultrasonography, we set the sound velocity at 1532 m/s (rather than the usual 1548 m/s, for a cataractous eye). However, even in the rare instances in which the posterior capsule is open, without fused walls, it is always necessary to have ciliary sulcus placement of secondary posterior chamber lenses because capsular bag fixation is practically impossible. Similarly, primary implants typically are not frequently used in children with bilateral cataracts who are younger than 3 or 4 years. Marked axial length changes during the first 2 years of life make it difficult to select the appropriate lens implant power for a very young eye. Bluestein and colleagues measured the size of the capsular bag in pediatric autopsy eyes. Wilson and associates have observed that capsular bag growth appears to stop after lensectomy, making lens decentration less of an issue. They argue that a posterior chamber in-the-bag placement is generally only possible with primary implants and carries lower risks of decentration and inflammation (due to contact with vascularized tissue). This anterior vault is less than in some earlier designs and with appropriate flexibility reduces the incidence of intermittent or persistent corneal touch. If the choice is between a larger or smaller lens, it is best to choose the larger one because current semiflexible lenses can accommodate slight oversizing. Put preplaced sutures in the sclera or limbus so that proper alignment is easier to achieve at the end of the case. By creating a taut diaphragm, miotics decrease the incidence of iris tuck and vitreous prolapse. When the anterior hyaloid face is intact but prolapsing into the anterior chamber, it can usually be pushed posteriorly by a bolus of sodium hyaluronate. Avoid injecting too much sodium hyaluronate because overfilling could make the iris diaphragm concave, predisposing to iris tuck. Perform an anterior vitrectomy if the hyaloid face is ruptured and if vitreous strands are incarcerated in the previous cataract wound. At the end of the vitrectomy, inject an air bubble into the anterior chamber to ascertain that the vitreous is back. To further ensure absence of vitreous strands to the wound, insert a spatula through a paracentesis to sweep over the iris plane while air is still in the anterior chamber. Grasp the lens by the tip, pass the lens across the anterior chamber, and position the inferior feet in the angle, avoiding extensive peripheral anterior synechia. Be careful to recognize and relieve iris tuck if it has occurred (it is indicated by a distorted pupil and can be relieved, if the lens is not too large, by rotating the lens). Also, pay attention to the location of previous iridectomies because haptics may rotate through them. A peripheral iridectomy is necessary if it is not already present from a previous cataract operation. Place the iridectomy far from the superior haptic to minimize haptic prolapse through the iridectomy. Kelman flexible, three-point fixation (b) and four-point fixation (c) lenses are popular designs for anterior chamber lenses. This strategy can also minimize the risk of vitreous loss through previously placed peripheral iridectomies, which are traditionally located superiorly. A surgeon may often have to consider a superior incision in a patient with such severe astigmatism that a temporal incision closed with nonabsorbable sutures would increase the magnitude of the astigmatism. Iritis and Hyphema Constant contact between the iris and the pseudophakos causes an inflammatory response, which may lead to recurrent microhyphema or gross hyphema. The incidence of this complication can be decreased by carefully sizing the secondary implants so that they are neither too large and erosive nor too small and excessively mobile. Acute or chronic glaucoma can develop after inadequate iridectomies or vitreous loss followed by implantation. Protect the corneal endothelium from injury during lens implantation by filling the anterior chamber with a high-molecular weight viscoelastic substance, such as sodium hyaluronate. At this step, a keratoscope can be used to adjust the knots to avoid surgically induced astigmatism. Move the spreader over the haptics and insert it between the claws from above, allowing the claws to be spread. With this risk in mind, patient selection is important because a patient with extremely damaged corneal endothelium could either forgo a secondary lens implantation or undergo a combined lens implantation and penetrating keratoplasty. A decrease in the number of normally functioning endothelial cells beyond the critical number needed to maintain corneal clarity is the cause of corneal endothelial decompensation.
Jose Barraquer (1958) demonstrated the dramatic efficacy of chemical zonulolysis using an enzyme a-chymotrypsin medicine prescription procyclidine 5 mg overnight delivery. The final significant improvement arrived when T Krawawicz in Poland (1961) introduced the cryoextractor 9 treatment issues specific to prisons cheap procyclidine on line. A miniature erysiphake with a small rubber suction bulb attached to the probe end illness and treatment discount 5 mg procyclidine with mastercard. Despite the encouraging results medicine used to stop contractions procyclidine 5 mg cheap, there remained a substantial rate of potentially blinding complications symptoms kidney infection buy procyclidine canada, including aphakic retinal detachment and cystoid macular edema, which could be reduced by keeping the posterior capsule intact. But the major concern was the optical rehabilitation of the aphakic patient with glasses. Few surgeons actually stuck to the technique because it was technically difficult and dangerous (high risk of corneal damage, capsular rupture, vitreous loss, and nucleus dislocation into the vitreous). The procedure also failed to catch on because a primary capsulotomy was taught, thus negating the advantage of compartmentalizing the anterior and posterior segments. While Kelman was developing his emulsification, John Shock (1972) introduced the alternative phacofragmentation and irrigation system. William Simcoe (1977) introduced his Simcoe curved 23-gauge cannula connected to a small irrigating bulb. In 1976, he introduced the simple low-flow double-bore irrigationaspiration cannula connected directly to a small aspirating syringe. Harold Scheie described a procedure for aspirating a soft congenital cataract from the eye through small incisions. He devised the technique of removing a window of anterior capsule with toothed forceps, by aspirating a soft nucleus or by expressing a hard nucleus, and by irrigating and aspirating a portion of the remaining cortex through a bent olive-tip cannula. The miotic pupil held the pedestal central until the loops stuck or scarred down to the posterior capsule. By 1977, Worst and colleagues reported on a large series of 2000 cases using this new lens. Kelman impressed an incredulous ophthalmic community by publishing his landmark description of the ultrasonic breakup of the nucleus coupled with the Scheie concept of irrigationaspiration of the cortex in 1967. Kelman was the invited guest of national medical meetings and showed films of his revolutionary work. He conducted courses at his local New York hospital and published an instruc- History of Cataract Surgery James Gills was also leading the way in Florida by performing high-volume surgery and perfecting the Gills method (with help from Robert Welch). The Gills method was a simple manual technique of nucleus expression followed by cortical cleanup with an end-opening Gills 25-gauge cannula attached to a 3-mm syringe. His cortical cleanup in a semiclosed chamber utilized the concept of engaging the cortex in the cannula port and then wiggling and teasing the cortex free from its capsular adherence. Repeated segments of cortex were teased out of the eye by cycles of insertion of the Gills needle with irrigation fluid, then suction and teasing of the cortex, and finally deliverance of the needle with the cortex out of the eye. The method was simple and effective, but automated systems gradually became more popular. Balazs in 1972 isolated and purified a hyaluronic acid gel for vitreous replacement. Emery and Little published a classic text that described with graphic detail their version of the KelmanCavitron phacoemulsifier-aspiration system. Surgeons were having second thoughts; why perform a procedure fraught with potential disasters Resurgence of interest in phacoemulsification came with a rapid succession of innovations. The first innovative idea to advance the safety of phacoemulsification was a new capsulotomy. The latter procedure proved to be the missing link to safe, in-the-bag nuclear emulsification. The technique of tearing a round hole in the anterior capsule was nothing short of brilliant. The next enhancement to phacoemulsification came through the evolution of ways to achieve nucleus manipulation and disassembly. In the early 1970s, Sinskey employed a one-handed technique to bowl out the central nucleus, followed by collapsing down and aspiration of the peripheral nuclear shell. Surgeons went to observe and learn from Kratz, and he became at that time the surgeon to operate on fellow ophthalmologists. A prized pupil, Maloney, traveled the country teaching the Kratz tilting technique. The learning curve was difficult, and surgeons were not happy with their frequent ruptured capsules, dropped nuclei, and damaged endothelium. The core concept was to create vertical forces to fragment the nucleus by burying a sharp-tipped chopping instrument into the anterior nucleus in front of the phaco tip and then pushing the chopper downwards while the phaco tip lifts upwards. White Star by Sovereign, Allergan delivers extremely brief ultrasound bursts interrupted by rest intervals, significantly decreasing the amount of heat delivered to the surrounding tissues. However, only very soft cataracts could be successfully managed using this technique, and patients had to be maintained on long-term steroid drops for the treatment of induced uveitis as well as mydriatics to prevent puncture site closure. In the following years, different laser wavelengths were tried with little success. Many of the ultrasound techniques were adapted for this technology, while newer ones, notable among which was a prechopping technique taught by Kamman and Dodick, were developed. So far, these newer technologies seem to work best on softer grades of nuclear sclerosis. It involves the placement of a small impeller inside the capsular bag through a 1 mm capsulorrhexis which, by spinning, causes swelling of the bag and creates an endocapsular vortex flow that allows extraction of the cataract. The Staar Sonic Wave (Staar Surgical) was the first phacoemulsification machine to incorporate sonic energy, generated at much lower frequencies than ultrasonic ones, as an alternative to conventional phacoemulsification. NeoSonix and Torsional phacoemulsification (Alcon) is a newer hybrid modality which uses sonic-frequency oscillations that can be supplemented with standard high-frequency ultrasonic phacoemulsification. The cutting tip vibrates along its longitudinal axis within the irrigating sleeve, thereby emulsifying the lens material upon contact. AquaLase (Infiniti System, Alcon Laboratories) uses the principle of hydraulics and propels short bursts of warmed balanced salt solution against lens material. This action appears to have no effect elsewhere in the eye, and does not dissipate radiating ultrasonic pressure waves. Frown incision for minimizing induced astigmatism after small incision cataract surgery with rigid optic intraocular lens implantation. Early in 1982, Kraff and Sanders proved that smaller incisions were better than large, producing less earlyinduced astigmatism and less late-healing astigmatic shift. Shepherd contributed a large breakthrough with the astigmatically neutral horizontal suture. The next advance to phacoemulsification was the revolutionary concept of moving the incision to clear cornea. Fine in February 1992 described a new concept of a planar temporal clear-corneal sutureless incision,77 which was a self-sealing incision positioned farthest away from the corneal center on the temporal meridian. Others recognized the elegant simplicity of the clear-corneal incision and ventured their modifications. During the evolution into phacoemulsification, there were some surgeons who for various reasons decided not to follow. They reported a series of 53 cases and found that phaco time, overall surgical time, total fluid use, and endothelial cell loss were comparable with those measured with their standard phaco techniques. Using an irrigating chopper and a bare phaco needle, he was able to perform bimanual phacoemulsification through a 0. In 1999, Crozafon of Nice, France coated the phaco tip with Teflon postulating that the poor thermal conductivity of the material would prevent thermal burns. Tsuneoka of Tokyo reported the use of a standard ultrasonic phacoemulsification for lens extraction through a 1. The current progress in microincisions, endocapsular vortex emulsification and injectable liquid lenses,91,92 all promising ingredients for such a surgery, brings the idea of a procedure in which lens removal through an anterior capsule puncture hole followed by reinflation of the bag with liquid lens material further from fiction and closer to reality. The future of crystalline lens surgery will continue to flourish in a competitive and stimulating environment in which surgeons and industry together work to advance the field. System of ophthalmology: diseases of the lens and vitreous; glaucoma and hypotomy, St Louis: Mosby; 1969:248264. Hirschberg J: the aspiration of a cataract, a radical operation by Arabian surgeons. Smith H: A new technique for the expression of the cataractous lens in its capsule. Knapp A: Report of one hundred successive extractions of cataract in the capsule after subluxation with the capsule forceps. Stoewer P: Demonstration eines Instruments zur Extraction der Linse in der Kapsel. Krawawicz T: Intracapsular extraction of intumescent cataract by application of low temperature. Ridley H: Intra-ocular acrylic lenses; a recent development in the surgery of cataract. Kratz R, Mazzocco T, Davidson B: the consecutive implantation of 250 Shearing intraocular lenses. Fankhauser F, Roussel P, Steffen J, et al: Clinical studies on the efficiency of high power laser radiation upon some structures of the anterior segment of the eye. First experiences of the treatment of some pathological conditions of the anterior segment of the human eye by means of a Q-switched laser system. Small-incision cataract surgery: foldable lenses, one-stitch surgery, sutureless surgery, astigmatic keratotomy. Masket S: Horizontal anchor suture closure method for small incision cataract surgery. Agarwal A, Agarwal S, Agarwal A: Phakonit and laser phakonit: lens removal through a 0. Tsuneoka H, Shiba T, Takahashi Y: Feasibility of ultrasound cataract surgery with a 1. Phaco chop: mastering techniques, optimizing technology, and avoiding complications. Paul T, Braga-Mele R: Bimanual microincisional phacoemulsification: the future of cataract surgery On 29 Nov 1949, Ridley carried out his first lens implantation on a 45-year-old woman. Problems that led to complications over the years following surgery were generally due to the crude operating techniques of the time. Modifications of implantation techniques were introduced in the early 1950s by Parry, while Epstein used this time to modify lens designs. Photographs of two autopsy eyes with Ridley lenses (image taken from the vitreous to the posterior lens surface and ciliary body: (a) right eye; (b) left eye). It was also possible for the haptics to erode in the ciliary body, leading to chronic uveitic reactions. The design principle of the open haptic loops was developed further in later years, both in anterior and posterior chamber lenses. The lens could be fixated in the anterior chamber following intra- or extracapsular cataract extraction. A further distinction can be drawn in the latter group, namely lenses with open or closed haptic loops. Within a short number of years, a multitude of different lenses appeared on the market. The main complication of the early anterior chamber lenses was corneal decompensation, which frequently appeared postoperatively. The constant contact to the corneal endothelium would lead to this problem years after surgery. Bad manufacturing techniques, residues on the lenses from the sterilization process and fundamental design flaws frequently led to serious inflammatory reactions and erosion of the fixation elements in the uvea structures. This lens was further developed in the Maltese cross lens and later the Copeland lens. During the early 1960s Jan Worst from the Netherlands developed his irisfixated lens. The medallion lens included fixation holes in the optic rim area, through which stitches were used to sew the lens into the iris. Worst finally conceived a new concept for iris fixation with the iris claw lens (lopster claw). Through two slits in both haptics, the lens was clamped into the mid-iris periphery tissue. The reputation of this lens was negatively influenced through unlicensed copies from other manufacturers during the 1970s. Copies offered lenses polished on a substandard level with sharp edges at the foot plates. Lenses with closed haptic loops ultimately led to considerable complications ranging from corneal decomposition to pronounced uveitic reactions. Binkhorst recognized that through this manner a significantly more stable fixation could be reached. With the introduction of microsurgery through Harms and Mackensen in the 1960s, a new era for microsurgery of the eyes began. A further group represents special developments, some of which were used in implantation surgery, others reaching a dead-end during the experimental stage itself, and yet others underwent modifications or developments. The looped haptics were first made using flexible materials such as polypropylene (prolene).
Histopathologically medicine 5325 purchase procyclidine us, arterial occlusion has been described with subendothelial cell infiltration of large retinal vessels by lymphoma cells medicine cabinets surface mount procyclidine 5 mg buy. Multiple left ocular creamy to white deep retinal lesions medications used to treat anxiety procyclidine 5 mg fast delivery, the smallest ones probably representing a subretinal pigment epithelial location 2 medications that help control bleeding procyclidine 5 mg buy on line. Note the indistinct retinal linear infiltrates treatment jiggers order discount procyclidine on-line, a vitritis, and an inferotemporal shallow retinal detachment. Note the clumping of the retinal pigment epithelium at the periphery of the lesion. Note that several of the discrete subunits at the periphery have an annular shape, shown particularly well at the left edge of the process. Uveitis accompanied by neurologic symptoms should prompt early consideration of the diagnosis. Cytology of the malignant cell in the vitreous is large, pleomorphic with scanty basophilic cytoplasm. The nuclei are big, round or oval, frequently indented, and may have segmented or clover-leaf configurations. The macrophages have delicate vesicular nucleoplasm without coarse clumping of the chromatinic material and more abundant and conspicuous cytoplasm. Massive collections of histiocytes such as these may be seen in infectious endophthalmitis, including toxoplasmic retinochoroiditis. When they are seen in profusion, they can be confused with primary ocular lymphoma. Note that the choroid is minimally thickened by inflammation but not involved with the lymphomatous process. The neoplastic lymphocytes are at least twice as large as the reactive lymphocytes in the choroid. Note the benign character of the small lymphocytes that have mounted a host response in the choroid. No brain lesions were detected originally, and neither a vitrectomy nor a biopsy was performed. The patient is being followed closely for any evidence of ocular progression or emergence of central nervous system lesions. Hyperchromatic neoplastic lymphocytes in the vitreous of a most exceptional case that did not have any identifiable masses in the retina. Hemorrhagic and partially necrotic brain lesion in a patient with ocular lymphoma. Since this patient had both eye and brain lymphoma, a multicentric origin is suggested. These pleomorphic lymphocytes have been stained by the immunoperoxidase method for the presence of lambda light chain determinants. Note that most cells in the underlying choroid are not staining positively, although there is a light dispersion of some B cells. Intraocular Lymphoproliferations Simulating Uveitis increase of the oncoprotein, is a well-known mechanism in the genesis of B-cell lymphoma. The translocation of the immunoglobulin heavy chain gene on chromosome 14 and bcl-2 gene on chromosome 18 often occurs in B-cell lymphoma. The visual acuity is often better than would be expected based on the clinical examination,8 which reveals primarily noninflammatory malignant cells in the vitreous. In a series of 44 patients, Cassoux and colleagues found punctate hyperfluorescent window defects in 54. Other less common findings included pigment epithelial detachments and punctate hyperfluorescent lesions. In 13 patients with ocular lymphoma, ultrasound included vitreous debris (77%), choroidalscleral thickening (46%), widening of the optic nerve (31%), elevated chorioretinal lesions (23%), and retinal detachment (15%). Systemic diffuse large B-cell lymphoma is comprised of germinal center B-cell, activated B-cell, and primary mediastinal B-cell groups. Migration of lymphocyte subsets into different sites is essential for normal immune function. Chemokines, a family of chemotactic cytokines, have been shown to direct the migration of leukocytes during inflammation and homing. These chemokines strongly attract B lymphocytes while promoting migration of only small numbers of T cells and macrophages. Beneath the retinal detachment shown toward the right are three small hillocks of thickening. The scan on the left running from top to bottom in the region of these hillocks shows minimal internal reflectivity. Dense sheets of vitreous cells in an older patient with neurologic symptoms is also highly suggestive of this diagnosis. In one study, the most common general symptoms were due to increased intracranial pressure (headache, nausea), seizures, and behavioral changes while the most common focal findings were hemiparesis, ataxia, and cranial nerve palsies. Vitreous specimens should be handled with care to protect the often fragile lymphoma cells. Sometimes it may be helpful to add tissue-culture medium in the vitrectomy specimen in the operating room. Computed tomographic scans of brain masses brought out after the injection of contrast material. In some cases in which diagnosis is not made on cytological examination of the vitreous, biopsy of retinal or subretinal infiltrates may be considered by a transvitreal or transscleral route. If the diagnostic vitrectomy is negative, then a repeated vitrectomy may be necessary or a biopsy of subretinal infiltrates should be appropriately elected. With therapy, survival improves substantially, but prognosis for long-term survival is still not optimal. In 1988, Freeman and colleagues reported that the median survival time with therapy, from onset of symptoms to death, is 35 months. Such lesions are less specific for lymphoma and also can be seen in sarcoidosis, multiple sclerosis, and systemic hypertension. Progression of the lesion shown in (a) over a 6-week period into that shown in (b) resulted in threatening of the macula retinae and necessitated ocular radiotherapy. In this case, the tumor infiltrated the nerve head, and radiation therapy merely disclosed the underlying damage on disappearance of the lesional tissue. Therefore, chemotherapy alone is the initial treatment of choice in older patients. An oncologist will treat the patient with close ocular monitoring by an ophthalmologist. At the International Central Nervous System & Ocular Lymphoma Workshop in 2004, the National Eye Institute and National Cancer Institute agreed to try to create an infrastructure to support an international network that would study key aspects such as the elucidation of basic mechanisms, diagnostics, and therapy of this devastating disease. Cases of ocular lymphoma secondary to systemic disease usually present with clinical signs and symptoms of anterior uveitis. Cases of systemic lymphoma presenting with a focal choroidal mass simulating a primary ocular melanoma clinically (as well as on fluorescein angiography and ultrasonography) or developing an optic nerve head mass with central artery occlusion have been described. Sometimes, ocular symptoms and signs are not related to tumor cells but rather opportunistic infections of the eye. On the basis of immunohistochemical characteristics, these cells are B-cell neoplastic cells. Secondary or metastatic lymphomatous involvement of the eye must be clearly distinguished conceptually from leukemic infiltration. Because of widespread vascular dissemination with elevated neoplastic white cell counts in the peripheral blood, leukemic cells have access to virtually every tissue and organ of the body. Clinical findings in acute myeloid leukemia usually involves the retina and presents as pseudo-Roth spots, retinal hemorrhages and perivascular infiltrates. In this enucleated globe, note the massive thickening of the choroid posteriorly and the two bulbous expansions of the ciliary body shown above. The arrow points to a smaller fish-egg-like component of the process that is located in the subretinal space. Note that both posteriorly and anteriorly, there is episcleral extension of tumor cells. Note that the eye is essentially quiet, belying the possibility that the condition is caused by an infection. The patient received 4000 cGy of ocular radiotherapy, and the condition completely resolved. The lesions are erythematous flat patches, often involving the lower torso and legs. Chemotherapy and radiation therapy are still popular for the treatment of systemic lymphoma. In the background, there are many mature lymphocytes and a scattering of eosinophilic leukocytes. Leukemic infiltration of the choroid has caused a disturbance of the retinal pigment epithelium, which has assumed linear, stellate, and leopard-spot-like aggregations. T-cell lymphomas, especially involving the eyelids, are the most common ophthalmic finding. Psoralen and ultraviolet A radiation may also be combined with a low dose of interferonalpha to treat later stages. In enucleated eyes of advanced cases, diffuse thickening of the uveal tract, particularly the choroid, occurs. The morphology of the cellular infiltrate appears benign, and lymphoid follicles with germinal centers are common. Most reported diagnoses have been based on histopathologic examination of enucleated eyes in advanced stages of the disease. Ultrasonography confirms choroidal thickening and demonstrates intact sclera in regions of extraocular extension with few internal acoustic interfaces owing to an absence of fibrous tissue. Less than 5% of choroidal malignant lymphomas present with diffuse choroidal infiltration, and within this variant, there is still an associated localized mass in 61% of patients. Clinical improvement with corticosteroid therapy is not characteristic of melanoma. The iris has been spared in this case (as it frequently is), but there is a small amount of retrobulbar and episcleral lymphoid extension below. The tumor cells have more ample cytoplasm than lymphocytes but retain the small dark nuclei of lymphocytes and therefore are referred to as lymphoplasmacytoid cells. Visual signs and symptoms include decreased acuity, cortical blindness, small white retinal or choroidal infiltrates, retinal pigmentary changes, retinal arterial occlusion, retinal hemorrhages, retinal vascular sheathing, vitritis, iridocyclitis, and keratic precipitates. Intravascular lymphomatosis has also been identified in association with concurrent carcinoma, diabetes mellitus, and chronic steroid use. In the absence of clinical improvement after such therapy, reconsideration of the diagnosis is appropriate. In patients intolerant of corticosteroid therapy, fractionated local external beam radiotherapy in modest doses (10002000 cGy) has been effective. Although a couple of the reported patients developed some evidence of systemic involvement, none died of this disease during a median follow-up period of 7 years and ranging to 39 years. Intravascular lymphomatosis (also called angiotrophic lymphoma and formerly referred to as malignant angioendotheliomatosis). This proliferation of large atypical lymphocytes has a predilection for the lumina of small arteries, veins, and capillaries, typically in the absence of overt peripheral blood or bone marrow disease. Neurologic and cutaneous presentations are common, with a minority of patients having clinically significant eye lesions. Extravascular infiltrates, usually seen at autopsy, are also observed in many organs, including the eye, orbit, pancreas, thyroid, and adrenal glands, but these infiltrates tend not to create large masses. Similar vascular changes are seen in the extraocular muscles, orbital nerves, and optic nerve. The tumor cells in most cases are of B-cell lineage, although a minority has been established to be of T-cell lineage. Ocular symptoms usually occur somewhat later and less predictably with disease progression. Biopsy of involved skin, meninges, and visceral organs may help to establish the diagnosis. Report of the Clinical Advisory Committee meeting, Airlie House, Virginia, November, 1997. Rosenwald A, Wright G, Leroy K, et al: Molecular diagnosis of primary mediastinal B cell lymphoma identifies a clinically favorable subgroup of diffuse large B cell lymphoma related to Hodgkin lymphoma. Shimoyama M, Oyama A, Tajima K, et al: Differences in clinicopathological characteristics and major prognostic factors between B-lymphoma and peripheral T-lymphoma excluding adult T-cell leukemia/lymphoma. Corriveau C, Easterbrook M, Payne D: Lymphoma simulating uveitis (masquerade syndrome). Cassoux N, MerleBeral H, Leblond V, et al: Ocular and central nervous system lymphoma: clinical features and diagnosis. MerleBeral H, Davi F, Cassoux N, et al: Biological diagnosis of primary intraocular lymphoma. Natural history based on a clinicopathologic study of eight cases and review of the literature. Presentation as retinal detachment with demonstration of monoclonal immunoglobulin light chains on the vitreous cells. Lobo A, Lightman S: Vitreous aspiration needle tap in the diagnosis of intraocular inflammation. Montesinos-Rongen M, Kuppers R, Schluter D, et al: Primary central nervous system lymphomas are derived from germinal-center B cells and show a preferential usage of the V4-34 gene segment. Pezzella F, Jones M, Ralfkiaer E, et al: Evaluation of bcl-2 protein expression and 14;18 translocation as prognostic markers in follicular lymphoma. Rossi D, Gaidano G: Molecular heterogeneity of diffuse large B-cell lymphoma: implications for disease management and prognosis. Durig J, Schmucker U, Duhrsen U: Differential expression of chemokine receptors in B cell malignancies.
Prepare a standard posterior chamber lens medicine 831 purchase procyclidine 5 mg with amex, preferably one with open loops and a length of at least 13 medicine natural buy 5 mg procyclidine with visa. However treatment pink eye 5 mg procyclidine buy otc, if the pupil is not adequately dilated treatment rheumatoid arthritis purchase procyclidine 5 mg online, dilate it to evaluate the condition of the capsule and to look for synechiae between the posterior surface of the iris and the capsule medicine joji procyclidine 5 mg low price. This material enlarges the posterior chamber to permit insertion of the distal footplate of the lens. Insert the distal loop of the lens into the posterior chamber nasally, between the iris and the capsule. Lens centration is easier if one applies preoperative laser marks at the sites where the claws should be anchored to the iris (as described previously). Even if the lens is properly centered intraoperatively, decentration may occur, and the lens may luxate either spontaneously or secondary to trauma if the fixation bite is too shallow. Sometimes, the surgeon can dissect some of the adhesions with a blunt spatula or fine microscissors. In the rare instance of an intact posterior capsule, the surgeon must determine whether the capsule is clear or hazy. Before closing the limbal incision, attempt to remove most of the viscoelastic from the anterior chamber. This can be achieved by injecting an air bubble into the nasal aspect of the anterior chamber, thereby pushing the viscoelastic material out of the eye. Alternatively, a vitrector on minimal infusion can be used to remove the viscoelastic gently from the eye. Perform a superotemporal iridotomy if there is not already a patent iridotomy or if the iris is bulging on either side of the implant. Another advantage of positioning the lens closer to the nodal point and center of rotation of the eye is the superior optical properties accrued by the lens in this position. Although it was more commonly seen with the earlier planar haptics, it occurs less frequently now with the more flexible haptics. The visual blurring evident in these cases resembles transient ischemic amaurosis. Alteration of the BloodAqueous Barrier After long-term contact with uveal tissue, polypropylene loops may flake or crack and become rough. The roughened loop surface could then chafe the posterior iris and liberate iris pigment. The integrity of the bloodaqueous barrier relies on intact surfaces of the iris and ciliary body, and this trauma to the iris has been hypothesized to lead to alteration of the bloodaqueous barrier with the subsequent release of inflammatory mediators. The surgeon can thus decrease the risk of hemorrhage, retinal detachment, and lens malposition by avoiding the potential inaccuracies of suture placement that are inherent to the ab externo technique. The basic surgical technique for an ab externo sulcus fixation of a posterior chamber secondary lens follows: 1. Pass the needle tip through the sulcus and behind the iris until it is visualized behind the pupil. Insert the straight needle into the barrel of the 28-gauge needle and withdraw the syringe from the eye (the syringe will carry with it the straight needle and suture). A taut segment of 100 polypropylene remains in the eye, extending from sulcus to sulcus. Cut the loop of suture, and securely tie one end to the superior haptic and the other to the inferior haptic. Slide the lens into the sulcus, and rotate it into position while removing slack from the attached sutures. Also, the decreased stability of the onepoint fixation of the sutures to the sclera allows for occasional lens decentration. Prepare the eye preoperatively in the usual fashion by maximally dilating the pupil and applying a Honan pressure cuff to diminish vitreous volume. Place a 40 silk bridle suture at the insertion of the superior rectus muscle to stabilize the eye. Bisect a 6-inch double-armed 100 polypropylene suture with standard needle, and tie the two free ends of the suture to the apex of each haptic using several square knots. One-point fixation to the sclera (a) provides less support than two-point fixation (b). Apply gentle counterpressure with the forceps externally while passing the suture through the sclera. After entering the anterior chamber with a sharp paracentesis knife, it is often necessary to perform a moderately extensive anterior vitrectomy with a mechanical vitrector. Viscoelastic is then injected into the anterior chamber to coat the corneal endothelium and to displace any residual vitreous posteriorly. Grasp the tip of the superior haptic with an angled McPherson forceps, then rotate the haptic over the optic while the forceps tip depresses the optic posteriorly. Once the elbow of the haptic is below the iris, direct it toward the ciliary sulcus by pronating the hand holding the angled forceps. Pass each needle through the half-thickness sclera 1 mm posterior to the exit site, leaving a loop in the suture so that the suture can be tied to itself. Leave the suture ends ~2 mm long so that they will lie flat under the conjunctiva, which is then sewn over the knot using 80 chromic suture. By using a smaller incision, surgeons can decrease the risk of intraocular fluid loss and hypotony, thereby improving globe stability during lens insertion and suturing. With a smaller incision, patients often achieve an earlier recovery of visual function and better preservation of corneal shape. By obviating the need for limbal-incision suturing, the small-incision Secondary Intraocular Lens Implantation the corneal wound and allowed to fall under the iris temporally. Permanently tie down the sutures into the bed of the scleral flap in the following manner: first create a loop; use the needles already present on the two ends to make a small, partial-thickness scleral pass adjacent to the exiting suture. The difficulty of the second step, in which the surgeon inserts the needle in the reverse position, from the inside out, might be alleviated by a trick that the author describes. Use a lens dialer to capture and pull the suture through the corneal incision, thereby creating a loop in the suture. Using a needle holder, curve the straight needles, and pass them through the sclera beneath the flaps. Cut the sutures long so that the ends do not erode the scleral flaps and conjunctiva. Erylidirim describes some tricks that may be helpful during two difficult steps of this procedure. First, it is often hard to find the entrance port while inserting the needle in reverse position. Before inserting the needle into the eye to make a port, mark the entrance point with a preinked marking pad. Touch the needle with the ink pad, and when the needle passes through the sclera, ink will remain on the surface of the sclera, leaving a blue circle with a hole in the center. Close the two superior sclerotomies, and leave the inferotemporal infusion in position, but turned off. Use a 4-mm keratome to create a small self-sealing, clear corneal incision near the temporal aspect of the limbus. With the needle holder, grasp a single double-armed 100 polypropylene suture with a straight needle on one end. By folding and inserting the lens in this fashion, the leading haptic remains in the proper orientation throughout the maneuver. The trailing haptic rotates 180° during unfolding and is not advanced through the corneal wound until after the lens is unfolded in the eye. From Ahmet E: Knotless scleral fixation for implanting a posterior chamber intraocular lens. Prepare the eye in the usual fashion, including the removal of vitreous from the anterior chamber, iris plane, and anterior vitreous cavity. Pass the other needle of the double-armed suture on a similar path, but exit the eye ~1 mm lateral to the first exit site. Rotate the needles backward through the pupil and behind the iris so that they exit through the superior ciliary sulcus. After closing the corneoscleral limbal wound in the usual fashion, close the scleral flaps at their corners with an 80 or 9. However, significant improvements in lens design and materials as well as changes in surgical technique have made pars plana fixation an acceptable surgical approach. The pars plana is relatively avascular and lies anterior to the retina; thus, one can avoid hemorrhagic complications and retinal detachments by making incisions through the sclera and choroid into the vitreous at the level of the pars plana. Pass a double-armed suture on a long needle through the incision, the pupil, under the iris, through the ciliary sulcus, and out through the sclera 11. The other needle of the double-armed suture is passed in a similar manner, exiting 1 mm lateral to the first exit site. The diameter of the lens must be increased to ~17 mm, and the diameter of the biconvex optic to 7 mm. If the lens is in this position, the A constant should be in the same range as for in-the-bag placement. Alternative methods of burying the knots include covering them with scleral flaps or a scleral groove. Therefore, to enter the pars plana safely, the sclera should be entered 35 mm behind the limbus, keeping the needle path parallel to the iris plane. Alternatively, they could be placed in a limbus-parallel position; both at the same distance from the limbus, but 2 mm apart. In either case, it is important to place these double sutures exactly opposite each other relative to the center of the cornea to avoid lens tilt. Teichmann notes that for greater stability, the two sutures attached to the haptic can be secured with two eyelets inferotemporally, at a distance of ~3 or 3. The haptic should then be secured with the single eyelet and one suture by creating iris-parallel stitches inserted at 3 and 3. Suture ends are tied and cut at the paracentesis and the iris pushed back into place. The main incision is closed after removal of viscoelastic material Recent work by Benevento and colleagues82 have suggested the added step of a safety net suture that is temporarily fixed in the posterior chamber to act as a surrogate capsule. The addition of this one step prior to lens insertion would facilitate the remainder of the procedure while potentially rendering it safer. Anterior vitrectomy if necessary for any vitreous remnant in the anterior chamber 3. Haptics inserted into ciliary sulcus and optic capture by pupil is induced (injection of intracameral myotic will facilitate this step). The haptics will be outlined against the posterior surface of the iris Optic Suture Fixation to Iris this technique involves fixing the optic rather than the haptic to the iris. The sutures are hooked and tied through a paracentesis adjacent to the needle exit sites after the needles are cut off 9. The two curved needles are passed through superior iris adjacent to the incision and tied to anterior iris surface 10. Intraocular hemorrhage is another possible complication that can be reduced by minimizing iris manipulation and paying close attention to needle placement during suturing. A range between 9% and 36% of patients with scleral-sutured lenses and penetrating keratoplasty experience this complication. The two important factors affecting the likelihood of iris chafe are suture location and tightness of the suture. The central iris is most mobile, therefore, central suture placement will result in excessive inflammation, but the fixing of central iris at sites of suture fixation will result in an irregular pupil with peaking at those sites. Excessively tight sutures or excessively large bites of Glaucoma Glaucoma is another common complication of scleral-sutured posterior chamber lens implants. Glaucoma after an implantation occurs even more frequently when the operation is performed at the same time as penetrating keratoplasty. Holland and colleagues suspected that scleral-sutured lenses were associated with glaucoma. Lens Decentration Lens tilt or decentration is found in 510% of patients after scleral-sutured posterior chamber lens implantation. The patients must be carefully informed about the possible risk of decreased vision and of complications during the procedure. The variety of methods of intraocular implantation allows the surgeon to individualize the approach to best fit each case. Choroidal Detachment Transscleral sutures are thought to increase the risk of choroidal detachment. Bellucci R, Pucci V, Morselli S, Bonomi L: Secondary implantation of angle-supported anterior chamber and scleral-fixated posterior chamber intraocular lenses. Hayashi K, Hayashi H, Nakao F, Hayashi F: Corneal endothelial cell loss in phacoemulsification surgery with silicone intraocular lens implantation. Hannush S: Sutured posterior chamber intraocular lenses: indications and procedures. Miyake K, Asakura M, Kobayashi H: Effect of intraocular lens fixation on the blood-aqueous barrier. Sasaharan M, Kiryu J, Yoshimura N: Endoscopic-assisted transcleral suture fixation to reduce the incidence of intraocular lens dislocation. Erylidirim A: Knotless scleral fixation for implanting a posterior chamber intraocular lens. The first wound closure attempt was by Desmarres in 1858, by means of an intact conjunctival bridge. Postoperative astigmatism was accepted as a natural consequence of cataract surgery.
Chlorambucil-induced seizures medications osteoarthritis pain procyclidine 5 mg buy low price, especially in children with nephrotic syndrome medicine 5513 purchase 5 mg procyclidine with amex, can occur symptoms 8 weeks purchase procyclidine 5 mg overnight delivery. Prophylactic trimethoprim/sulfamethoxazole is often recommended and long-term antiviral therapy may be needed medications and pregnancy discount procyclidine 5 mg mastercard. Other toxicities include possible demyelinating disease treatment 001 procyclidine 5 mg purchase with mastercard, drug-induced lupus, neutropenia, and abnormal liver function. Otherwise, a definite increase in malignancies has not been proven with this class of medication. For patients with ankylosing spondylitis, prospective studies indicate that either etanercept or infliximab may markedly reduce episodes of acute anterior uveitis. In addition to local reactions at the injection site, side effects have included granulomatous inflammation. Rituximab has been an available therapy for many years to treat lymphomas that express this marker. More recently it has demonstrated efficacy in the treatment of either rheumatoid arthritis or systemic lupus erythematosus. It produces a sustained depletion of B cells and clinical efficacy tends to be maintained for about a year. Its role in the treatment of ocular inflammatory disease has not been extensively studied. Interferon beta is a widely prescribed approach to the treatment of multiple sclerosis, for example. Although this drug is available to treat rheumatoid arthritis, its efficacy has been modest. However, anakinra is dramatically effective for a family of rare, autosomal dominant diseases that include familial cold urticaria, Muckle-Wells syndrome, and neonatal onset multisystem disease. These diseases are known as autoinflammatory syndromes because of the spontaneous onset of inflammation in the absence of detectable auto-antibodies. Cytokines that are currently being inhibited in clinical trials for diseases like psoriasis and rheumatoid arthritis include interleukin-6, interleukin-15, and interleukin12/23. Progress in the sustained release of intraocular therapies offers the potential that some of these approaches could be used locally in order to achieve efficacy comparable to intravitreally administered corticosteroid while avoiding the rampant toxicities of cataract and glaucoma from local corticosteroids. Alternatively stated, both the physician and patient need to recognize the risk/benefit ratio of the approach. We also subscribe to the philosophy that the least amount of medication is the best amount of medication. This is a controversial philosophy among uveitis specialists with some clinicians preferring to eliminate all evidence of inflammation. Clinical judgment must surely be invoked to determine when the risk of increased medication is justified by the amount of inflammation present. In an idealized setting, the treatment succeeds in eliminating all traces of inflammation. In practice, some compromise is usually made between the risk of the medication and the potential benefit to be achieved. With these caveats in mind, the vast majority of patients with uveitis can benefit from therapy that suppresses the inflammatory response. Infectious causes of uveitis may cause masquerade syndromes which must be recognized and treated appropriately. For those patients whose disease is apparently caused by a harmful immune response, therapy can usually be tailored to reduce the damage from inflammation while allowing acceptable risk from the suppression of the immune system. Segal R, Mozes E, Yaron M, Tartakovsky B: the effects of methotrexate on the production and activity of interleukin-1. Constantin A, Loubet-Lescoulie P, Lambert N, et al: Antiinflammatory and immunoregulatory action of methotrexate in the treatment of rheumatoid arthritis: evidence of increased interleukin-4 and interleukin-10 gene expression demonstrated in vitro by competitive reverse transcriptase-polymerase chain reaction. Farber S, Diamond L, Mercer R: Temporary remissions in acute leukaemia in children produced by folic antagonist, 4aminopteroyl-glutamic acid. Bom S, Zamiri P, Lightman S: Use of methotrexate in the management of sightthreatening uveitis. Kaplan-Messas A, Barkana Y, Avni I, Neumann R: Methotrexate as a first-line corticosteroid-sparing therapy in a cohort of uveitis and scleritis. Rau R, Herborn G: Benefit and risk of methotrexate treatment in rheumatoid arthritis. Sterneck M, Fischer L, Gahlemann C, et al: Mycophenolate mofetil for prevention of liver allograft rejection: initial results of a controlled clinical trial. Glicklich D, Acharya A: Mycophenolate mofetil therapy for lupus nephritis refractory to intravenous cyclophosphamide. Filler G, Hansen M, LeBlanc C, et al: Pharmacokinetics of mycophenolate mofetil for autoimmune disease in children. Maddison P, Kiely P, Kirkham B, et al: Leflunomide in rheumatoid arthritis: recommendations through a process of consensus. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in immunoregulatory disorders. Johnston A, Belitsky P, Frei U, et al: Potential clinical implications of substitution of generic cyclosporine formulations for cyclosporine microemulsion (Neoral) in transplant recipients. Bachmann K, Jauregui L, Chandra R, Thakker K: Influence of a 3-day regimen of azithromycin on the disposition kinetics of cyclosporine A in stable renal transplant patients. Boissonnat P, de Lorgeril M, Perroux V, et al: A drug interaction study between ticlopidine and cyclosporin in heart transplant recipients. Guba M, von Breitenbuch P, Steinbauer M, et al: Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: involvement of vascular endothelial growth factor. Ikeda E, Hikita N, Eto K, Mochizuki M: Tacrolimus-rapamycin combination therapy for experimental autoimmune uveoretinitis. Braun J, Baraliakos X, Listing J, Sieper J: Decreased incidence of anterior uveitis in patients with ankylosing spondylitis treated with the anti-tumor necrosis factor agents infliximab and etanercept. Uveitis can also be classified clinically according to the type of uveitis (Table 92. Earlier classification systems divide uveitis into granulomatous and nongranulomatous as well as acute and chronic. Acute uveitis affecting the front of the eye normally presents with redness (usually in a circumcorneal distribution), pain, photophobia, and a small reduction in visual acuity. The inflammatory response causes white blood cells such as neutrophils, monocytes, and lymphocytes, to leave the inflamed iris vessels to enter the aqueous humor. The aqueous humor becomes sticky, causing the iris to adhere in various places to the adjacent anterior capsule of the lens, known as posterior synechiae, which leads to a small, odd-shaped pupil. Often a sign of impending iris bombé will be easily visible through dilated iris blood vessels. The iris has a smooth appearance with blunting of crypts, a dull stroma and loss of crispness of iris architecture. A characteristic feature of herpes viral uveitis is sector iris atrophy with iris transillumination and a dilated, often eccentric, pupil. They are seen as tiny refractile deposits within the iris stroma on slit-lamp examination. Careful scanning of the iris is essential as the crystals are normally seen only when the slit beam is at a certain angle. They are thought to represent unusually large Russell bodies that are spherical immunoglobulins containing structures derived from plasma cells. Russell bodies occur as a result of a block in the normal pathways of immunoglobulin secretion within plasma cells. Normally it is the posterior subcapsular type, but nuclear sclerotic cataract (often with rapid progression and the development of index myopia) may also occur. Cataract formation may also result from corticosteroid therapy or a combination of corticosteroid and inflammation. Severe anterior chamber inflammation can result in some spillover of cells into the anterior vitreous. Part of the examination should include a search for conjunctival follicles, a feature of ocular sarcoidosis, that are most often found in the tarsal conjunctiva. Factors in the history and examination that one should be aware of are shown in Tables 92. Rates of uveitis were higher in women than men, both for new and prevalent cases and interestingly an increased incidence was found with advancing age with the highest rates seen in the population over the age of 65 peaking at 102. Anterior uveitis is the most common form of uveitis in most Western countries, accounting for 5092% of total uveitis cases, as compared to 2850% in Asian countries. There is a high frequency of recurrence with a highly variable interval between attacks, usually ~14 25 months. Inflammation is usually nongranulomatous but in severe cases can cause a plasmoid aqueous with a fibrin clot or a hypopyon. A minority of cases may involve the posterior segment secondarily, leading to vision-threatening complications such as cystoid macular edema, vitreitis, retinal vasculitis, papillitis, or pars planitis. The organisms implicated include Chlamydia trachomatis, Klebsiella, Yersinia, Shigella, and Salmonella species, and Campylobacter jejuni. Nevertheless, much of the evidence is indirect and involves the detection of humoral and cellular immune responses to various bacteria. In a series of 31 patients with unilateral anterior uveitis with sectoral iris atrophy and without previous keratitis,22 there was a high female-to-male ratio (22:9) with an average age at onset of 39 years (range 879 years). Ocular hypertension was always observed in association with cells in the anterior chamber during a period of inflammatory activity. Treatment is aimed at dampening down the inflammatory response and preventing recurrence. In the acute attack topical corticosteroids are given and a mydriatic (if appropriate). The latter may not be necessary as the pupil may be dilated as a result of the iris atrophy. The topical corticosteroids are then tapered in frequency and potency to the weakest preparation possible and to prevent recurrence, such as prednisolone 0. If recurrences still occur then an oral antiviral, such as aciclovir can be added. Systemic corticosteroids are indicated for bilateral macular edema in patients who cannot tolerate or do not respond to periocular corticosteroids. Patients on long-term therapy are kept on the minimum possible medication to control the inflammation to minimize the side effects of corticosteroids in cataract and secondary glaucoma. Pupillary dilation may be required at night to keep the pupil mobile and prevent formation of posterior synechiae. Sarcoidosis and the seronegative spondyloarthropathies were the most common systemic disease associations identified. Uveitis involved only the anterior segment in 80% of cases and was bilateral at presentation in 77% of cases. Patients were treated with systemic corticosteroids in 80% of cases and with immunosuppressive drugs in 9% of cases. Uveitis recurred or followed a chronic course in 56% of patients and persisted for several years in some cases. Prevention of recurrence appears possible using oral ganciclovir or its prodrug, valganciclovir,24,25,27 and one case has been treated with intravitreal ganciclovir. Over the past three decades the distinctions between adult and childhood arthritis have became more defined, yet the European and North American classifications of childhood arthritis have diverged. Although no correlation existed between activity of joint and eye inflammation, an association between the mode of onset of juvenile arthritis and subsequent risk of uveitis was recognized by both sets of criteria: systemic onset (with features such as quotidian (daily) fever, hepatosplenomegaly, lymphadenopathy, or rash) carried the lowest risk, and the pauciarticular onset, the highest. The incidence had been reported as up to 21%3436 with 6789% of these being bilateral. Loss of vision has been reported in up to 66% patients, with ocular complications, such as band keratopathy, glaucoma, posterior synechiae, cataract, maculopathy, and pthisis bulbi in 75%. Slitlamp examination typically reveals only an occasional small nonpigmented keratic precipitate on the corneal endothelium with a mild anterior uveitis (+0. This is an acute interstitial nephritis, which is thought to be an immune-mediated process that can be drug-related, infectionrelated, or idiopathic and can account for 1015% of patients with acute renal failure. It often presents with nonspecific constitutional symptoms, such as fever and flank tenderness. Laboratory investigations reveal an elevated serum creatinine, proteinuria, hematuria, and a sterile pyuria. A renal biopsy is required to make the definitive diagnosis, and shows edema in the renal interstitium with predominantly mononuclear infiltrate of activated T-cells, plasma cells, and histiocytes. Laboratory abnormalities included elevated erythrocyte sedimentation rates and urinary b-2-microglobulin levels. It defined clinically homogeneous subgroups of disease, in the hope that hitherto obscured underlying etiologic and pathogenetic factors would emerge to improve the understanding of the disease process. The oligoarthritis group was further subcategorized into persistent (affecting no more than four joints throughout the disease course), or extended (affecting a cumulative total of five joints or more after the first 6 months of disease) categories. This model was not good in predicting which patient would develop uveitis (sensitivity 55%, specificity 26%). Anterior Uveitis and extended oligoarthritis subgroups, although in larger numbers in the former. However, in many uveitis patients, routine investigations, serological and radiological, are often of not much help. Usually there are no serological markers of disease activity which can be found in patients with systemic vasculitis. Also, any abnormalities found in peripheral blood may not reflect what is going on inside the eye. Nevertheless, in view of the puzzling nature of uveitis and that it may form part of a systemic disease process, many patients are investigated, as it is important not to miss a readily treatable cause.
Generic procyclidine 5 mg online. Fibromyalgia symptoms - why you should never ignore frequent headaches.
References
- Castro DJ, Sridhar KS, Garewal HS, et al. Intratumoral cisplatin/epinephrine gel in advanced head and neck cancer: a multi- center, randomized, double-blind, phase III study in North America. Head Neck 2003;25:717-731.
- Terhaard C, Lubsen H, Rasch C, et al. The role of radiotherapy in the treatment of malignant salivary gland tumors. Int J Radiat Oncol Biol Phys 2009;61:103-111.
- De Meerleer G, Fonteyne V, Meersschout S, et al: Salvage intensity-modulated radiotherapy for rising PSA after radical prostatectomy, Radiother Oncol 89(2):205n213, 2008.
- Care N, Young GB, Doig G, et al. Anoxic ischemic encephalopathy: clinical and electrophysiological associations with outcome. Neurocrit Care. 2005;2(2):159-164.
- Wallentin L, et al, for the PLATO Investigators: Tricagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009;361:1045-1057.
- Arkinstall, W., Sandler, A., Goughnour, B., Babul, N., Harsanyi, Z., & Darke, A. C. (1995). Efficacy of controlled-release codeine in chronic non-malignant pain: A randomized, placebo-controlled clinical trial. Pain, 62(2), 169n178.
- Kohl SK, Mathews K, Baker J: Renal hilar mass in an 85-year-old woman. Solitary fibrous tumor, Arch Pathol Lab Med 130(1):117n119, 2006.
- Hess CP, Fullerton HJ, Metry DW, et al: Cervical and intracranial arterial anomalies in 70 patients with PHACE syndrome, AJNR Am J Neuroradiol 31(10):1980-1986, 2010.