
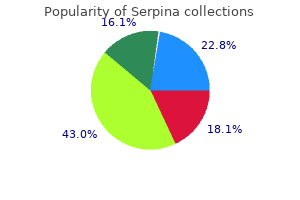
Serpina
| Contato
Página Inicial
Robert Arntfield, MD
- Assistant Professor of Medicine, Divisions of Emergency Medicine and Critical Care Medicine, Western University, London Health Sciences Centre, London, Ontario, Canada
Functionally selective agonists are thought to occupy the orthosteric ligandbinding site anxiety symptoms jelly legs serpina 60 caps purchase without prescription, making their binding competitive with conventional Well-Established Second Messengers A anxiety symptoms tinnitus buy serpina 60 caps otc. It also regulates the production of adrenal and sex steroids (in response to corticotropin or follicle-stimulating hormone) anxiety while sleeping cheap serpina 60 caps without prescription, relaxation of smooth muscle anxiety xiphoid process cheapest serpina, and many other endocrine and neural processes anxiety girl purchase online serpina. Milrinone, a selective inhibitor of type 3 phosphodiesterases that are expressed in cardiac muscle cells, has been used as an adjunctive agent in treating acute heart failure. Some of the hormones, neurotransmitters, and growth factors that trigger this pathway bind to receptors linked to G proteins, whereas others bind to receptor tyrosine kinases. If agonist is removed after a short time (typically several to tens of minutes, indicated by broken line on abscissa), cells recover full responsiveness to a subsequent addition of agonist (second light-colored bar). This "resensitization" fails to occur, or occurs incompletely, if cells are exposed to agonist repeatedly or over a more prolonged time period. B: Agonist binding to receptors initiates signaling by promoting receptor interaction with G proteins (Gs) located in the cytoplasm (step 1 in the diagram). The receptor-arrestin complex binds to coated pits, promoting receptor internalization (step 3). Repeated or prolonged exposure of cells to agonist favors the delivery of internalized receptors to lysosomes (step 6), promoting receptor down-regulation rather than resensitization. With its multiple second messengers and protein kinases, the phosphoinositide signaling pathway is much more complex than calcium-sensitive protein kinase called protein kinase C. For example, different cell types may contain one or more specialized calcium- and calmodulin-dependent kinases with limited substrate specificity (eg, myosin light-chain kinase) in addition to a general calcium- and calmodulindependent kinase that can phosphorylate a wide variety of protein substrates. Furthermore, at least nine structurally distinct types of protein kinase C have been identified. These and other nonreceptor elements of the calciumphosphoinositide signaling pathway are of considerable importance in pharmacotherapy. For example, lithium ion, used in treatment of bipolar (manic-depressive) disorder, affects the cellular metabolism of phosphoinositides (see Chapter 29). A number of useful vasodilating drugs, such as nitroglycerin and sodium nitroprusside used in treating cardiac ischemia and acute hypertension, act by generating or mimicking nitric oxide. One such drug is sildenafil, used in treating erectile dysfunction and pulmonary hypertension (see Chapter 12). Isolation of Signaling Mechanisms the opposite of signal interplay is seen in some situations-an effective isolation of signaling according to location in the cell. For example, calcium signaling in the heart is highly localized because calcium released into the cytoplasm is rapidly sequestered by nearby calcium-binding proteins and is locally pumped from the cytoplasm into the sarcoplasmic reticulum. Phosphorylation: A Common Theme Almost all second messenger signaling involves reversible phosphorylation, which performs two principal functions in signaling: amplification and flexible regulation. In flexible regulation, differing substrate specificities of the multiple protein kinases regulated by second messengers provide branch points in signaling pathways that may be independently regulated. Inhibitors of protein kinases have great potential as therapeutic agents, particularly in neoplastic diseases. Trastuzumab, an antibody that antagonizes growth factor receptor signaling (discussed earlier), is a useful therapeutic agent for breast cancer. Another example of this general approach is imatinib, a small molecule inhibitor of the cytoplasmic tyrosine kinase Abl, which is activated by growth factor signaling pathways. Imatinib is effective for treating chronic myelogenous leukemia, which is caused by a chromosomal translocation event that produces an active Bcr/Abl fusion protein in hematopoietic cells. Thus, if a series of related agonists exhibits identical relative potencies in producing two distinct effects, it is likely that the two effects are mediated by similar or identical receptor molecules. In addition, if identical receptors mediate both effects, a competitive antagonist will inhibit both responses with the same Ki; a second competitive antagonist will inhibit both responses with its own characteristic Ki. Thus, studies of the relation between structure and activity of a series of agonists and antagonists can identify a species of receptor that mediates a set of pharmacologic responses. Exactly the same experimental procedure can show that observed effects of a drug are mediated by different receptors. In this case, effects mediated by different receptors may exhibit different orders of potency among agonists and different Ki values for each competitive antagonist. Wherever we look, evolution has created many different receptors that function to mediate responses to any individual chemical signal. In some cases, the same chemical acts on completely different structural receptor classes. In addition, each structural class usually includes multiple subtypes of receptor, often with significantly different signaling or regulatory properties. For example, many biogenic amines (eg, norepinephrine, acetylcholine, histamine, and serotonin) activate more than one receptor, each of which may activate a different G protein, as previously described (see also Table 21). The existence of many receptor classes and subtypes for the same endogenous ligand has created important opportunities for drug development. For example, propranolol, a selective antagonist of adrenoceptors, can reduce an accelerated heart rate without preventing the sympathetic nervous system from causing vasoconstriction, an effect mediated by 1 adrenoceptors. Different cell types express different accessory proteins, which interact with steroid receptors and change the functional effects of drug-receptor interaction. For example, tamoxifen is a drug that binds to steroid receptors naturally activated by estrogen. Tamoxifen acts as an antagonist on estrogen receptors expressed in mammary tissue but as an agonist on estrogen receptors in bone. Consequently, tamoxifen may be useful not only in the treatment of breast cancer but also in the prevention of osteoporosis by increasing bone density (see Chapters 40 and 42). Tamoxifen may create complications in postmenopausal women, however, by exerting an agonist action in the uterus, stimulating endometrial cell proliferation. New drug development is not confined to agents that act on receptors for extracellular chemical signals. Increasingly, pharmaceutical chemists are determining whether elements of signaling pathways distal to the receptors may also serve as targets of selective and useful drugs. We have already discussed drugs that act on phosphodiesterase and some intracellular kinases. When faced with a patient who needs treatment, the prescriber must make a choice among a variety of possible drugs and devise a dosage regimen that is likely to produce maximal benefit and minimal toxicity. To make rational therapeutic decisions, the prescriber must understand how drug-receptor interactions underlie the relations between dose and response in patients, the nature and causes of variation in pharmacologic responsiveness, and the clinical implications of selectivity of drug action. Graded Dose-Response Relations To choose among drugs and to determine appropriate doses of a drug, the prescriber must know the relative pharmacologic potency and maximal efficacy of the drugs in relation to the desired therapeutic effect. Potency of a drug depends in part on the affinity (Kd) of receptors for binding the drug and in part on the efficiency with which drug-receptor interaction is coupled to response. Note that some doses of drug A can produce larger effects than any dose of drug B, despite the fact that we describe drug B as pharmacologically more potent. The reason for this is that drug A has a larger maximal efficacy (as described below). For therapeutic purposes, the potency of a drug should be stated in dosage units, usually in terms of a particular therapeutic end point (eg, 50 mg for mild sedation, 1 mcg/kg/min for an increase in heart rate of 25 bpm). Maximal efficacy-This parameter reflects the limit of the dose-response relation on the response axis. Thus, diuretics that act on one portion of the nephron may produce much greater excretion of fluid and electrolytes than diuretics that act elsewhere. Extremely steep dose-response curves (eg, curve D) may have important clinical consequences if the upper portion of the curve represents an undesirable extent of response (eg, coma caused by a sedative-hypnotic). Steep dose-response curves in patients can result from cooperative interactions of several different actions of a drug (eg, effects on brain, heart, and peripheral vessels, all contributing to lowering of blood pressure). In an idealized in vitro system, efficacy denotes the relative maximal efficacy of agonists and partial agonists that act via the same receptor. In therapeutics, efficacy denotes the extent or degree of an effect that can be achieved in the intact patient. Thus, therapeutic efficacy may be affected by the characteristics of a particular drug-receptor interaction, but it also depends on a host of other factors as noted in the text. Quantal Dose-Effect Curves Graded dose-response curves of the sort described above have certain limitations in their application to clinical decision making. For example, such curves may be impossible to construct if the pharmacologic response is an either-or (quantal) event, such as prevention of convulsions, arrhythmia, or death. Furthermore, the clinical relevance of a quantitative dose-response relation in a single patient, no matter how precisely defined, may be limited in application to other patients, owing to the great potential variability among patients in severity of disease and responsiveness to drugs. The specified quantal effect may be chosen on the basis of clinical relevance (eg, relief of headache) or for preservation of safety of experimental subjects (eg, using low doses of a cardiac stimulant and specifying an increase in heart rate of 20 bpm as the quantal effect), or it may be an inherently quantal event (eg, death of an experimental animal). When these responses are summated, the resulting cumulative frequency distribution constitutes a quantal dose-effect curve (or dose-percent curve) of the proportion or percentage of individuals who exhibit the effect plotted as a function of log dose. Shaded boxes (and the accompanying bell-shaped curves) indicate the frequency distribution of doses of drug required to produce a specified effect; that is, the percentage of animals that required a particular dose to exhibit the effect. The open boxes (and the corresponding colored curves) indicate the cumulative frequency distribution of responses, which are lognormally distributed. Quantal dose-effect curves may also be used to generate information regarding the margin of safety to be expected from a particular drug used to produce a specified effect. One measure, which relates the dose of a drug required to produce a desired effect to that which produces an undesired effect, is the therapeutic index. The precision possible in animal experiments may make it useful to use such a therapeutic index to estimate the potential benefit of a drug in humans. Of course, the therapeutic index of a drug in humans is almost never known with real precision; instead, drug trials and accumulated clinical experience often reveal a range of usually effective doses and a different (but sometimes overlapping) range of possibly toxic doses. The range between the minimum toxic dose and the minimum therapeutic dose is called the therapeutic window and is of greater practical value in choosing the dose for a patient. The clinically acceptable risk of toxicity depends critically on the severity of the disease being treated. For example, the dose range that provides relief from an ordinary headache in the majority of patients should be very much lower than the dose range that produces serious toxicity, even if the toxicity occurs in a small minority of patients. Critical information required for making rational therapeutic decisions can be obtained from each type of curve. Both curves provide information regarding the potency and selectivity of drugs; the graded dose-response curve indicates the maximal efficacy of a drug, and the quantal dose-effect curve indicates the potential variability of responsiveness among individuals. Occasionally, individuals exhibit an unusual or idiosyncratic drug response, one that is infrequently observed in most patients. The idiosyncratic responses are usually caused by genetic differences in metabolism of the drug or by immunologic mechanisms, including allergic reactions. Quantitative variations in drug response are, in general, more common and more clinically important. An individual patient is hyporeactive or hyperreactive to a drug in that the intensity of effect of a given dose of drug is diminished or increased compared with the effect seen in most individuals. When responsiveness diminishes rapidly after administration of a drug, the response is said to be subject to tachyphylaxis. Even before administering the first dose of a drug, the prescriber should consider factors that may help in predicting the direction and extent of possible variations in responsiveness. These include the propensity of a particular drug to produce tolerance or tachyphylaxis as well as the effects of age, sex, body size, disease state, genetic factors, and simultaneous administration of other drugs. Four general mechanisms may contribute to variation in drug responsiveness among patients or within an individual patient at different times. Alteration in Concentration of Drug That Reaches the Receptor As described in Chapter 3, patients may differ in the rate of absorption of a drug, in distributing it through body compartments, or in clearing the drug from the blood. By altering the concentration of drug that reaches relevant receptors, such pharmacokinetic differences may alter the clinical response. Some differences can be predicted on the basis of age, weight, sex, disease state, and liver and kidney function, and by testing specifically for genetic differences that may result from inheritance of a functionally distinctive complement of drug-metabolizing enzymes (see Chapters 4 and 5). Variation in Concentration of an Endogenous Receptor Ligand this mechanism contributes greatly to variability in responses to pharmacologic antagonists. Thus, propranolol, a -adrenoceptor antagonist, markedly slows the heart rate of a patient whose endogenous catecholamines are elevated (as in pheochromocytoma) but does not affect the resting heart rate of a well-trained marathon runner. Alterations in Number or Function of Receptors Experimental studies have documented changes in drug response caused by increases or decreases in the number of receptor sites or by alterations in the efficiency of coupling of receptors to distal effector mechanisms. In some cases, the change in receptor number is caused by other hormones; for example, thyroid hormones increase both the number of adrenoceptors in rat heart muscle and cardiac sensitivity to catecholamines. Similar changes probably contribute to the tachycardia of thyrotoxicosis in patients and may account for the usefulness of propranolol, a -adrenoceptor antagonist, in ameliorating symptoms of this disease. In other cases, the agonist ligand itself induces a decrease in the number (eg, down-regulation) or coupling efficiency (eg, desensitization) of its receptors. These mechanisms (discussed previously under Signaling Mechanisms & Drug Action) may contribute to two clinically important phenomena: first, tachyphylaxis or tolerance to the effects of some drugs (eg, biogenic amines and their congeners), and second, the "overshoot" phenomena that follow withdrawal of certain drugs. An antagonist may increase the number of receptors in a critical cell or tissue by preventing downregulation caused by an endogenous agonist. When the antagonist is withdrawn, the elevated number of receptors can produce an exaggerated response to physiologic concentrations of agonist. Potentially disastrous withdrawal symptoms can result for the opposite reason when administration of an agonist drug is discontinued. In this situation, the number of receptors, which has been decreased by drug-induced down-regulation, is too low for endogenous agonist to produce effective stimulation. For example, the withdrawal of clonidine (a drug whose 2-adrenoceptor agonist activity reduces blood pressure) can produce hypertensive crisis, probably because the drug down-regulates 2 adrenoceptors (see Chapter 11). The study of genetic factors determining drug response is called pharmacogenetics, and the use of gene sequencing or expression profile data to tailor therapies specific to an individual patient is called personalized or precision medicine. For example, somatic mutations affecting the tyrosine kinase domain of the epidermal growth factor receptor in lung cancers can confer enhanced sensitivity to kinase inhibitors such as gefitinib. This effect enhances the antineoplastic effect of the drug, and because the somatic mutation is specific to the tumor and not present in the host, the therapeutic index of these drugs can be significantly enhanced in patients whose tumors harbor such mutations. Genetic analysis can also predict drug resistance during treatment or identify new targets for therapy based on rapid mutation of the tumor in the patient.
These properties have made it a popular "club drug" that goes by colorful street names such as "liquid ecstasy anxiety related disorders 60 caps serpina sale," "grievous bodily harm anxiety job 60 caps serpina order free shipping," or "date rape drug anxiety 911 buy 60 caps serpina fast delivery. It is rapidly absorbed after ingestion and reaches a maximal plasma concentration 2030 minutes after ingestion of a 1020 mg/kg dose anxiety herbs purchase serpina 60 caps fast delivery. They induce anxiety symptoms worse in morning discount 60 caps serpina overnight delivery, often in an unpredictable way, perceptual symptoms, including shape and color distortion. Psychosis-like manifestations (depersonalization, hallucinations, distorted time perception) have led some to classify these drugs as psychotomimetics. They also produce somatic symptoms (dizziness, nausea, paresthesias, and blurred vision). Some users have reported intense reexperiencing of perceptual effects (flashbacks) up to several years after the last drug exposure. Hallucinogens differ from most other drugs described in this chapter in that they induce neither dependence nor addiction. However, repetitive exposure still leads to rapid tolerance (also called tachyphylaxis). Animals do not self-administer hallucinogens, suggesting that they are not rewarding to them. After synthesis, blotter paper or sugar cubes are sprinkled with the liquid and allowed to dry. During this time, subjects have impaired ability to make rational judgments and understand common dangers, which puts them at risk for accidents and personal injury. Nicotine exposure occurs primarily through smoking of tobacco, which causes associated diseases that are responsible for many preventable deaths. When nicotine excites projection neurons, dopamine is released in the nucleus accumbens and the prefrontal cortex, thus fulfilling the dopamine requirement of addictive drugs. These receptors are mainly expressed on synaptic terminals of excitatory afferents projecting onto the dopamine neurons. They also contribute to nicotine-evoked dopamine release and the long-term changes induced by the drugs related to addiction (eg, long-term synaptic potentiation of excitatory inputs). Nicotine withdrawal is mild compared with opioid withdrawal and involves irritability and sleep problems. However, nicotine is among the most addictive drugs (relative risk 4), and relapse after attempted cessation is very common. Treatment Treatments for nicotine addiction include nicotine itself in forms that are slowly absorbed and several other drugs. Nicotine that is chewed, inhaled, or transdermally delivered can be substituted for the nicotine in cigarettes, thus slowing the pharmacokinetics and eliminating the many complications associated with the toxic substances found in tobacco smoke. Varenicline may impair the capacity to drive and has been associated with suicidal ideation. Many countries have banned smoking in public places to create smoke-free environments. This important step not only reduces passive smoking and the hazards of secondhand smoke, but also the risk that ex-smokers will be exposed to smoke, which as a contextual cue, may trigger relapse. Benzodiazepine dependence is very common, and diagnosis of addiction is probably often missed. Withdrawal from benzodiazepines occurs within days of stopping the medication and varies as a function of the half-life of elimination. Symptoms include irritability, insomnia, phonophobia and photophobia, depression, muscle cramps, and even seizures. Because of this difference, unitary synaptic currents in interneurons are larger than those in dopamine neurons, and when this difference is amplified by benzodiazepines, interneurons fall silent. By extension, 1-sparing compounds, which at present remain experimental and are not approved for human use, may eventually be preferred to treat anxiety disorders because of their reduced risk of induced addiction. Barbiturates, which preceded benzodiazepines as the most commonly abused sedative-hypnotics (after ethanol), are now rarely prescribed to outpatients and therefore constitute a less common prescription drug problem than they did in the past. Management of barbiturate withdrawal and addiction is similar to that of benzodiazepines. Although only a minority becomes dependent and addicted, abuse is a very serious public health problem because of the social costs and many diseases associated with alcoholism. They represent a definite risk for abuse, which has to be weighed against their beneficial effects. Some persons abuse Pharmacology the pharmacology of alcohol is complex, and no single receptor mediates all of its effects. It is not clear which of these targets is responsible for the increase of dopamine release from the mesolimbic reward system. Dependence becomes apparent 612 hours after cessation of heavy drinking as a withdrawal syndrome that may include tremor (mainly of the hands), nausea and vomiting, excessive sweating, agitation, and anxiety. In some individuals, this is followed by visual, tactile, and auditory hallucinations 1224 hours after cessation. Finally, 4872 hours after cessation, an alcohol withdrawal delirium (delirium tremens) may become apparent in which the person hallucinates, is disoriented, and shows evidence of autonomic instability. Surprisingly, intravenous administration of ketamine can eliminate episodes of depression within hours (see Chapter 30), which is in strong contrast to selective serotonin reuptake inhibitors and other antidepressants, which usually take weeks to act. Regardless, a limitation is the transient nature of the effect, which wears off within days even with repetitive administration. These substances are present in a variety of household and industrial products that are inhaled by "sniffing," "huffing," or "bagging. It is common for novices to start with sniffing and progress to huffing and bagging as addiction develops. Altered function of ionotropic receptors and ion channels throughout the central nervous system has been demonstrated for a few. Other substances, such as amyl nitrite ("poppers"), primarily produce smooth muscle relaxation and enhance erection but are not addictive. With chronic exposure to the aromatic hydrocarbons (eg, benzene, toluene), toxic effects can be observed in many organs, including white matter lesions in the central nervous system. Treatment Treatment of ethanol withdrawal is supportive and relies on benzodiazepines, taking care to use compounds such as oxazepam and lorazepam, which are not as dependent on oxidative hepatic metabolism as most other benzodiazepines. In patients in whom monitoring is not reliable and liver function is adequate, a longeracting benzodiazepine such as chlordiazepoxide is preferred. As in the treatment of all chronic drug abuse problems, heavy reliance is placed on psychosocial approaches to alcohol addiction. This is perhaps even more important for the alcoholic patient because of the ubiquitous presence of alcohol in many social contexts. The pharmacologic treatment of alcohol addiction is limited, although several compounds, with different goals, have been used. Both drugs, along with others, are now classified as "club drugs" and sold under names such as "angel dust," "Hog," and "Special K. The effects of these substances became apparent when patients undergoing surgery reported unpleasant vivid dreams and hallucinations after anesthesia. Psychedelic effects last for about 1 hour and also include increased blood pressure, impaired memory function, and visual alterations. Cocaine is highly addictive (relative risk = 5), and its use is associated with a number of complications. For more than 100 years, it has been extracted and used in clinical medicine, mainly as a local anesthetic and to dilate pupils in ophthalmology. Sigmund Freud famously proposed its use to treat depression and alcohol dependence, but addiction quickly brought an end to this idea. Cocaine hydrochloride is a water-soluble salt that can be injected or absorbed by any mucosal membrane (eg, nasal snorting). When heated in an alkaline solution, it is transformed into the free base, "crack cocaine," which can then be smoked. Inhaled crack cocaine is rapidly absorbed in the lungs and penetrates swiftly into the brain, producing an almost instantaneous "rush. This mechanism, underlying its effect as a local anesthetic, seems responsible for neither the acute rewarding nor the addictive effects. In the central nervous system, cocaine blocks the uptake of dopamine, noradrenaline, and serotonin through their respective transporters. Cocaine exposure increases the risk for intracranial hemorrhage, ischemic stroke, myocardial infarction, and seizures. The term "crack-baby" was used to describe a specific syndrome of the newborn, and the mothers faced harsh legal consequences. The follow-up of the children, now adults, does not confirm a drug-specific handicap in cognitive performance. Moreover, in this population, the percentage of drug-users is comparable to controls matched for socioeconomic environment. Susceptible individuals may become dependent and addicted after only a few exposures to cocaine. Although a withdrawal syndrome is reported, it is not as strong as that observed with opioids. Tolerance may develop, but in some users, a reverse tolerance is observed; that is, they become sensitized to small doses of cocaine. Cravings are very strong and underlie the very high addiction liability of cocaine. To date, no specific antagonist is available, and the management of intoxication remains supportive. Amphetamine, methamphetamine, and their many derivatives exert their effects by reversing the action of biogenic amine transporters at the plasma membrane. Similar mechanisms apply for other biogenic amines (serotonin and norepinephrine). They are often produced in small clandestine laboratories, which makes their precise chemical identification difficult. They differ from ecstasy chiefly in the context of use: intravenous administration and "hard-core" addiction are far more common with amphetamines, especially methamphetamine. In general, amphetamines lead to elevated catecholamine levels that increase arousal and reduce sleep, whereas the effects on the dopamine system mediate euphoria but may also cause abnormal movements and precipitate psychotic episodes. Effects on serotonin transmission may play a role in the hallucinogenic and anorexigenic functions as well as in the hyperthermia often caused by amphetamines. Amphetamines are typically taken initially in pill form by abusers, but can also be smoked or injected. Within hours after oral ingestion, amphetamines increase alertness and cause euphoria, agitation, and confusion. Effects on heart rate may be minimal with some compounds (eg, methamphetamine), but with increasing dosage these agents often lead to tachycardia and dysrhythmias. Withdrawal consists of dysphoria, drowsiness (in some cases, insomnia), and general irritability. With repetitive administration, serotonin depletion may become permanent, which has triggered a debate on its neurotoxicity. Other complications include serotonin syndrome (mental status change, autonomic hyperactivity, and neuromuscular abnormalities; see Chapter 16) and seizures. Withdrawal is marked by a mood "offset" characterized by depression lasting up to several weeks. This is particularly true in the case of a massive overdose, in which reversal of drug action may be a life-saving measure. Pharmacologic interventions may also aim to alleviate the withdrawal syndrome, particularly after opioid exposure. On the assumption that withdrawal reflects-at least in part-a hyperactivity of central adrenergic systems, the 2-adrenoceptor agonist clonidine (also used as a centrally active antihypertensive drug, see Chapter 11) has been used with some success to attenuate withdrawal. Today, most clinicians prefer to manage opioid withdrawal by very slowly tapering the administration of long-acting opioids. Another widely accepted treatment is substitution of a legally available agonist that acts at the same receptor as the abused drug. For example, heroin addicts may receive methadone to replace heroin; smoking addicts may receive nicotine continuously via a transdermal patch system to replace smoking. In general, a rapidacting substance is replaced with one that acts or is absorbed more slowly. Substitution treatments are largely justified by the benefits of reducing associated health risks, the reduction of drugassociated crime, and better social integration. This is perhaps not surprising, because the main effect of ecstasy appears to be to foster feelings of intimacy and empathy without impairing intellectual capacities. Ecstasy therefore is the prototypic designer drug and, as such, is increasingly popular. Because of frequent adverse effects-most notably severe depression carrying a substantial risk of suicide-this drug is no longer used clinically. It was initially used in conjunction with diet and exercise for patients with a body mass index above 30 kg/m2 (27 kg/m2 if associated risk factors, such as type 2 diabetes or dyslipidemia, are present). Although a recent large-scale study confirmed that rimonabant is effective for smoking cessation and the prevention of weight gain in smokers who quit, this indication has never been approved. While the cellular mechanism of rimonabant remains to be elucidated, data in rodents convincingly demonstrate that this compound can reduce self-administration in naive as well as drug-experienced animals. Case studies seem to confirm the potential of such approaches, but controlled clinical studies are lacking. Refining deep brain stimulation to emulate optogenetic treatment of synaptic pathology. Maskos U et al: Nicotine reinforcement and cognition restored by targeted expression of nicotinic receptors. Pascoli V, Terrier J, Hiver A, Lüscher C: Sufficiency of mesolimbic dopamine neuron stimulation for the progression to addiction. Hallucinations are often caused by a cannabis overdose, especially when hashish is ingested.
Still higher concentrations of antagonist (curves D and E) reduce the number of available receptors to the point that maximal response is diminished anxiety symptoms throwing up 60 caps serpina otc. Here anxiety treatment discount generic serpina uk, maximal response is elicited by activation of relatively few receptors because the response initiated by an individual ligandreceptor-binding event persists longer than the binding event itself anxiety side effects discount serpina 60 caps with amex. Irrespective of the biochemical basis of receptor reserve anxiety guided meditation generic serpina 60 caps line, the sensitivity of a cell or tissue to a particular concentration of agonist depends not only on the affinity of the receptor for binding the agonist (characterized by the Kd) but also on the degree of spareness-the total number of receptors present compared with the number actually needed to elicit a maximal biologic response anxiety 800 numbers order serpina on line. The concept of spare receptors is very useful clinically because it allows one to think precisely about the effects of drug dosage without having to consider (or even fully understand) biochemical details of the signaling response. The Kd of the agonist-receptor interaction determines what fraction (B/Bmax) of total receptors will be occupied at a given free concentration (C) of agonist regardless of the receptor concentration: agonist present at a concentration equal to the Kd will occupy 50% of the receptors, and half of the effectors will be activated, producing a half-maximal response (ie, two receptors stimulate two effectors). Now imagine that the number of receptors increases tenfold to 40 receptors but that the total number of effectors remains constant. As a result, a much lower concentration of agonist suffices to occupy 2 of the 40 receptors (5% of the receptors), and this same low concentration of agonist is able to elicit a half-maximal response (two of four effectors activated). Thus, it is possible to change the sensitivity of tissues with spare receptors by changing receptor number. Competitive & Irreversible Antagonists Receptor antagonists bind to receptors but do not activate them; the primary action of antagonists is to reduce the effects of agonists (other drugs or endogenous regulatory molecules) that normally activate receptors. While antagonists are traditionally thought to have no functional effect in the absence of an agonist, some antagonists exhibit "inverse agonist" activity (see Chapter 1) because they also reduce receptor activity below basal levels observed in the absence of any agonist at all. Antagonist drugs are further divided into two classes depending on whether or not they act competitively or noncompetitively relative to an agonist present at the same time. In the presence of a fixed concentration of agonist, increasing concentrations of a competitive antagonist progressively inhibit the agonist response; high antagonist concentrations prevent the response almost completely. Here the number of effectors does not limit the maximal response, and the receptors are not spare in number. In the presence of a competitive antagonist, higher concentrations of agonist are required to produce a given effect; thus the agonist concentration (C) required for a given effect in the presence of concentration [I] of an antagonist is shifted to the right, as shown. The concentration (C) of an agonist required to produce a given effect in the presence of a fixed concentration ([I]) of competitive antagonist is greater than the agonist concentration (C) required to produce the same effect in the absence of the antagonist. The ratio of these two agonist concentrations (called the dose ratio) is related to the dissociation constant (Ki) of the antagonist by the Schild equation: C [l] =1+ C Ki Pharmacologists often use this relation to determine the Ki of a competitive antagonist. Even without knowledge of the relation between agonist occupancy of the receptor and response, the Ki can be determined simply and accurately. For the clinician, this mathematical relation has two important therapeutic implications: 1. The degree of inhibition produced by a competitive antagonist depends on the concentration of antagonist. Patients receiving a fixed dose of this drug exhibit a wide range of plasma concentrations, owing to differences among individuals in the clearance of propranolol. As a result, inhibitory effects on physiologic responses to norepinephrine and epinephrine (endogenous adrenergic receptor agonists) may vary widely, and the dose of propranolol must be adjusted accordingly. Clinical response to a competitive antagonist also depends on the concentration of agonist that is competing for binding to receptors. Again, propranolol provides a useful example: When this drug is administered at moderate doses sufficient to block the effect of basal levels of the neurotransmitter norepinephrine, resting heart rate is decreased. However, the increase in the release of norepinephrine and epinephrine that occurs with exercise, postural changes, or emotional stress may suffice to overcome this competitive antagonism. Accordingly, the same dose of propranolol may have little effect under these conditions, thereby altering therapeutic response. Conversely, the same dose of propranolol that is useful for treatment of hypertension in one patient may be excessive and toxic to another, based on differences between the patients in the amount of endogenous norepinephrine and epinephrine that they produce. The actions of a noncompetitive antagonist are different because, once a receptor is bound by such a drug, agonists cannot surmount the inhibitory effect irrespective of their concentration. In many cases, noncompetitive antagonists bind to the receptor in an irreversible or nearly irreversible fashion, sometimes by forming a covalent bond with the receptor. Therapeutically, such irreversible antagonists present distinct advantages and disadvantages. Once the irreversible antagonist has occupied the receptor, it need not be present in unbound form to inhibit agonist responses. Consequently, the duration of action of such an irreversible antagonist is relatively independent of its own rate of elimination and more dependent on the rate of turnover of receptor molecules. Phenoxybenzamine, an irreversible -adrenoceptor antagonist, is used to control the hypertension caused by catecholamines released from pheochromocytoma, a tumor of the adrenal medulla. If administration of phenoxybenzamine lowers blood pressure, blockade will be maintained even when the tumor episodically releases very large amounts of catecholamine. In this case, the ability to prevent responses to varying and high concentrations of agonist is a therapeutic advantage. If the -adrenoceptor blockade cannot be overcome, excess effects of the drug must be antagonized "physiologically," ie, by using a pressor agent that does not act via adrenoceptors. Such drugs are called negative allosteric modulators because they act through binding to a different (ie, "allosteric") site on the receptor relative to the classical (ie, "orthosteric") site bound by the agonist and reduce activity of the receptor. Not all allosteric modulators act as antagonists; some potentiate rather than reduce receptor activity. Benzodiazepines have little activating effect on their own, and this property is one reason that benzodiazepines are relatively safe in overdose; even at high doses, their ability to increase ion conductance is limited by the release of endogenous neurotransmitter. Allosteric modulation can also occur at targets lacking a known orthosteric binding site. Certain mutations that render the channel hypoactive can be partially rescued by ivacaftor, representing positive allosteric modulation of a channel for which there is no presently known endogenous ligand. It is important to emphasize that the failure of partial agonists to produce a maximal response is not due to decreased affinity for binding to receptors. This mixed "agonist-antagonist" property of partial agonists can have both beneficial and deleterious effects in the clinic. For example, buprenorphine, a partial agonist of -opioid receptors, is a generally safer analgesic drug than morphine because it produces less respiratory depression in overdose. However, buprenorphine is effectively antianalgesic when administered in combination with more efficacious opioid drugs, and it may precipitate a drug withdrawal syndrome in opioid-dependent patients. Other Mechanisms of Drug Antagonism Not all mechanisms of antagonism involve interactions of drugs or endogenous ligands at a single type of receptor, and some types of antagonism do not involve a receptor at all. For example, protamine, a protein that is positively charged at physiologic pH, can be used clinically to counteract the effects of heparin, an anticoagulant that is negatively charged. In this case, one drug acts as a chemical antagonist of the other simply by ionic binding that makes the other drug unavailable for interactions with proteins involved in blood clotting. Another type of antagonism is physiologic antagonism between endogenous regulatory pathways mediated by different receptors. For example, several catabolic actions of the glucocorticoid hormones lead to increased blood sugar, an effect that is physiologically opposed by insulin. Because the full agonist (blue line) and the partial agonist (green line) compete to bind to the same receptor sites, when occupancy by the partial agonist increases, binding of the full agonist decreases. B: When each of the two drugs is used alone and response is measured, occupancy of all the receptors by the partial agonist produces a lower maximal response than does similar occupancy by the full agonist. C: Simultaneous treatment with a single concentration of full agonist and increasing concentrations of the partial agonist produces the response patterns shown in the bottom panel. The fractional response caused by a single high concentration of the full agonist decreases as increasing concentrations of the partial agonist compete to bind to the receptor with increasing success; at the same time, the portion of the response caused by the partial agonist increases, while the total response-ie, the sum of responses to the two drugs (red line)-gradually decreases, eventually reaching the value produced by partial agonist alone (compare with B). In general, use of a drug as a physiologic antagonist produces effects that are less specific and less easy to control than are the effects of a receptor-specific antagonist. Thus, for example, to treat bradycardia caused by increased release of acetylcholine from vagus nerve endings, the physician could use isoproterenol, a -adrenoceptor agonist that increases heart rate by mimicking sympathetic stimulation of the heart. However, use of this physiologic antagonist would be less rational-and potentially more dangerous-than use of a receptor-specific antagonist such as atropine (a competitive antagonist of acetylcholine receptors that slow heart rate as the direct targets of acetylcholine released from vagus nerve endings). Most transmembrane signaling is accomplished by a small number of different molecular mechanisms. Each type of mechanism has been adapted, through the evolution of distinctive protein families, to transduce many different signals. These protein families include receptors on the cell surface and within the cell, as well as enzymes and other components that generate, amplify, coordinate, and terminate postreceptor signaling by chemical second messengers in the cytoplasm. This section first discusses the mechanisms for carrying chemical information across the plasma membrane and then outlines key features of cytoplasmic second messengers. Each represents a different family of receptor protein and uses a different strategy to circumvent the barrier posed by the lipid bilayer of the plasma membrane. We should also consider different structural families of receptor protein, and this allows us to ask basic questions with important clinical implications: · Why do some drugs produce effects that persist for minutes, hours, or even days after the drug is no longer present Intracellular Receptors for Lipid-Soluble Agents Several biologic ligands are sufficiently lipid-soluble to cross the plasma membrane and act on intracellular receptors. These "gene-active" receptors belong to a protein family that evolved from a common precursor. For example, binding of glucocorticoid hormone to its normal receptor protein relieves an inhibitory constraint on the transcription-stimulating activity of the protein. The mechanism used by hormones that act by regulating gene expression has two therapeutically important consequences: 1. All of these hormones produce their effects after a characteristic lag period of 30 minutes to several hours-the time required for the synthesis of new proteins. This means that the geneactive hormones cannot be expected to alter a pathologic state within minutes (eg, glucocorticoids will not immediately relieve the symptoms of bronchial asthma). The effects of these agents can persist for hours or days after the agonist concentration has been reduced to zero. The persistence of effect is primarily due to the relatively slow turnover of most enzymes and proteins, which can remain active in cells for hours or days after they have been synthesized. Consequently, it means that the beneficial (or toxic) effects of a geneactive hormone usually decrease slowly when administration of the hormone is stopped. The glucocorticoid receptor polypeptide is schematically depicted as a protein with three distinct domains. A heat-shock protein, hsp90, binds to the receptor in the absence of hormone and prevents folding into the active conformation of the receptor. Binding of a hormone ligand (steroid) causes dissociation of the hsp90 stabilizer and permits conversion to the active configuration. In all these receptors, the two domains are connected by a hydrophobic segment of the polypeptide that resides in the lipid bilayer of the plasma membrane. The resulting change in receptor conformation causes two receptor molecules to bind to one another (dimerize). This activates the tyrosine kinase enzyme activity present in the cytoplasmic domain of the dimer, leading to phosphorylation of the receptor as well as additional downstream signaling proteins. Activated receptors catalyze phosphorylation of tyrosine residues on different target signaling proteins, thereby allowing a single type of activated receptor to modulate a number of biochemical processes. The receptor polypeptide has extracellular and cytoplasmic domains, depicted above and below the plasma membrane. The cytoplasmic domains become phosphorylated (P) on specific tyrosine residues (Y), and their enzymatic activities are activated, catalyzing phosphorylation of substrate proteins (S). Insulin, for example, uses a single class of tyrosine kinase receptors to trigger increased uptake of glucose and amino acids and to regulate metabolism of glycogen and triglycerides in the cell. Activation of the receptor in specific target cells drives a complex program of cellular events ranging from altered membrane transport of ions and metabolites to changes in the expression of many genes. Inhibitors of particular receptor tyrosine kinases are finding increased use in neoplastic disorders in which excessive growth factor signaling is often involved. Some of these inhibitors are monoclonal antibodies (eg, trastuzumab, cetuximab), which bind to the extracellular domain of a particular receptor and interfere with binding of growth factor. Ligand binding often induces accelerated endocytosis of receptors from the cell surface, followed by the degradation of those receptors (and their bound ligands). This downregulation process is essential physiologically to limit the strength and duration of the growth factor signal; genetic mutations that interfere with the down-regulation process cause excessive and prolonged responses that underlie or contribute to many forms of cancer. Endocytosis of other receptor tyrosine kinases, most notably receptors for nerve growth factor, serves a very different function. Internalized nerve growth factor receptors are not rapidly degraded but are translocated in endocytic vesicles from the distal axon, where receptors are activated by nerve growth factor released from the innervated tissue, to the cell body. In the cell body, the growth factor signal is transduced to transcription factors regulating the expression of genes controlling cell survival. This process, effectively opposite to down-regulation, transports a critical survival signal from its site of agonist release to the site of a critical downstream signaling effect and can do so over a remarkably long distance-up to a meter in some neurons. Receptors in both groups, like the receptor tyrosine kinases, are active in their dimeric forms. Cytokine Receptors Cytokine receptors respond to a heterogeneous group of peptide ligands, which include growth hormone, erythropoietin, several kinds of interferon, and other regulators of growth and differentiation. These polypeptides, each of which crosses the lipid bilayer four times, form a cylindrical structure that is approximately 10 nm in diameter but is impermeable to ions. For ligand-gated ion channels, drugs often mimic or block the actions of natural agonists. Each of their receptors transmits its signal across the plasma membrane by increasing transmembrane conductance of the relevant ion and thereby altering the electrical potential across the membrane. One form of this receptor is a pentamer made up of four different polypeptide subunits (eg, two chains plus one, one, and one chain, all with molecular weights ranging from 43,00050,000). The receptor molecule is depicted as embedded in a rectangular piece of plasma membrane, with extracellular fluid above and cytoplasm below. The structural basis for activating other ligandgated ion channels has been determined recently, and similar general principles apply, but there are differences in key details that may open new opportunities for drug action. For example, receptors that mediate excitatory neurotransmission at central nervous system synapses bind glutamate, a major excitatory neurotransmitter, through a large appendage domain that protrudes from the receptor and has been called a "flytrap" because it physically closes around the glutamate molecule; the glutamate-loaded flytrap domain then moves as a unit to control pore opening. Drugs can regulate the activity of such glutamate receptors by binding to the flytrap domain, to surfaces on the membraneembedded portion around the pore, or within the pore itself. The time elapsed between the binding of the agonist to a ligand-gated channel and the cellular response can often be measured in milliseconds. The rapidity of this signaling mechanism is crucially important for moment-to-moment transfer of information across synapses.
Syndromes
- Urinalysis
- Apert syndrome
- Blisters or ulcers -- most often on the mouth, lips and gums, or genitals
- Barium swallow x-ray
- Memory loss
- Gastroesophageal reflux (GERD)
- Use a needle to draw fluid out of a cyst, which will be examined under a microscope to look for cancer cells
- Low body temperature (hypothermia)
- Bleeding (hemorrhage)
Central Nervous System Applications the amphetamines have a mood-elevating (euphoriant) effect; this effect is the basis for the widespread abuse of this drug group (see Chapter 32) anxiety rash 60 caps serpina order with mastercard. The amphetamines also have an alerting anxiety 025 60 caps serpina for sale, sleepdeferring action that is manifested by improved attention to repetitive tasks and by acceleration and desynchronization of the electroencephalogram anxiety symptoms wikipedia generic 60 caps serpina with mastercard. Modafinil anxiety psychiatrist safe 60 caps serpina, a new amphetamine substitute anxiety fear buy serpina 60 caps line, is approved for use in narcolepsy and is claimed to have fewer disadvantages (excessive mood changes, insomnia, and abuse potential) than amphetamine in this condition. Amphetamines have appetite-suppressing effects, but there is no evidence that long-term improvement in weight control can be achieved with amphetamines alone, especially when administered for a relatively short course. Some patients with this syndrome respond well to low doses of methylphenidate and related agents. Extended-release formulations of methylphenidate may simplify dosing regimens and increase adherence to therapy, especially in school-age children. Cotecchia S: the 1-adrenergic receptors: Diversity of signaling networks and regulation. Johnson M: Molecular mechanisms of 2-adrenergic receptor function, response, and regulation. Philipp M, Hein L: Adrenergic receptor knockout mice: Distinct functions of 9 receptor subtypes. Fenoldopam Hydroxyamphetamine Isoproterenol Metaraminol Methamphetamine Methylphenidate Midodrine Mirabegron Modafinil Naphazoline Norepinephrine Olodaterol Oxymetazoline Phenylephrine Pseudoephedrine Tetrahydrozoline Tizanidine Xylometazoline Iopidine Nuvigil Alphagan Precedex Focalin Generic, Dexedrine Generic, Dobutrex Generic, Intropin Northera Generic Generic, Adrenalin Chloride, Primatene Mist, Bronkaid Mist, EpiPen, Auvi-Q Corlopam Paremyd (includes 0. The best indicator of this is the profound drop in orthostatic blood pressure without an adequate compensatory increase in heart rate. Pure autonomic failure is a neurodegenerative disorder selectively affecting peripheral autonomic fibers. Conversely, these patients are hypersensitive to the pressor effects of agonists and other sympathomimetics. For example, the agonist midodrine can increase blood pressure significantly at doses that have no effect in normal subjects and can be used to treat their orthostatic hypotension. Caution should be observed in the use of sympathomimetics (including over-the-counter agents) and sympatholytic drugs. These became more severe and were eventually accompanied by throbbing headaches and drenching sweats. Physical examination revealed a blood pressure of 150/90 mm Hg and heart rate of 88 bpm. During the physical examination, palpation of the abdomen elicited a sudden and typical episode, with a rise in blood pressure to 210/120 mm Hg, heart rate to 122 bpm, profuse sweating, and facial pallor. What caused the blood pressure and heart rate to rise so high during the examination Catecholamines play a role in many physiologic and pathophysiologic responses, as described in Chapter 9. Drugs that block their receptors therefore have important effects, some of which are of great clinical value. The classification of adrenoceptors into 1, 2, and subtypes and the effects of activating these receptors are discussed in Chapters 6 and 9. Blockade of peripheral dopamine receptors is of limited clinical importance at present. For pharmacologic research, 1- and 2-adrenoceptor antagonist drugs have been very useful in the experimental exploration of autonomic function. In clinical therapeutics, nonselective antagonists are used in the treatment of pheochromocytoma (tumors that secrete catecholamines), and 1-selective antagonists are used in primary hypertension and benign prostatic hyperplasia. Beta-receptor antagonist drugs are useful in a much wider variety of clinical conditions and are firmly established in the treatment of hypertension, ischemic heart disease, arrhythmias, endocrinologic and neurologic disorders, glaucoma, and other conditions. Reversible antagonists dissociate from receptors, and the block can be surmounted with sufficiently high concentrations of agonists; irreversible drugs do not dissociate and cannot be surmounted. These drugs and labetalol-drugs used primarily for their antihypertensive effects-as well as several ergot derivatives (see Chapter 16) are also reversible -adrenoceptor antagonists or partial agonists. Brett English for improving tables, and our students at Vanderbilt for advice on conceptual clarity. As discussed in Chapters 1 and 2, the duration of action of a reversible antagonist is largely dependent on the half-life of the drug in the body and the rate at which it dissociates from its receptor: the shorter the half-life of the drug in the body, the less time it takes for the effects of the drug to dissipate. In contrast, the effects of an irreversible antagonist may persist long after the drug has been cleared from the plasma. In the case of phenoxybenzamine, the restoration of tissue responsiveness after extensive -receptor blockade is dependent on synthesis of new receptors, which may take several days. The rate of return of 1-adrenoceptor responsiveness may be particularly important in patients who have a sudden cardiovascular event or who become candidates for urgent surgery. This change in response is called epinephrine reversal; it illustrates how the activation of both and receptors in the vasculature may lead to opposite responses. Alpha-receptor antagonists often cause orthostatic hypotension and reflex tachycardia; nonselective (1 = 2, Table 101) blockers usually cause significant tachycardia if blood pressure is lowered below normal. Orthostatic hypotension is due to antagonism of sympathetic nervous system stimulation of 1 receptors in vascular smooth muscle; contraction of veins is an important component of the normal capacity to maintain blood pressure in the upright position since it decreases venous pooling in the periphery. Constriction of arterioles in the legs also contributes to the normal orthostatic response. Tachycardia may be more marked with agents that block 2-presynaptic receptors in the heart, since the augmented release of norepinephrine will further stimulate receptors in the heart. Other Effects Blockade of receptors in other tissues elicits miosis (small pupils) and nasal stuffiness. Alpha1 receptors are expressed in the base of the bladder and the prostate, and their blockade decreases resistance to the flow of urine. The tension produced in isolated strips of cat spleen, a tissue rich in receptors, was measured in response to graded doses of norepinephrine. Left: Tolazoline, a reversible blocker, shifted the curve to the right without decreasing the maximum response when present at concentrations of 10 and 20 mol/L. Right: Dibenamine, an analog of phenoxybenzamine and irreversible in its action, reduced the maximum response attainable at both concentrations tested. Epinephrine reversal is demonstrated by tracings showing the response to epinephrine before (middle) and after (bottom) phentolamine. Drugs Alpha antagonists Prazosin, terazosin, doxazosin Phenoxybenzamine Phentolamine Yohimbine, tolazoline Mixed antagonists Labetalol, carvedilol Beta antagonists Metoprolol, acebutolol, alprenolol, atenolol, betaxolol, celiprolol, esmolol, nebivolol Propranolol, carteolol, nadolol, penbutolol, pindolol, timolol Butoxamine 1 >>> 2 1 = 2 1 > 2 1 >>>> 2 1 > 2 1 = 2 2 >> 1 Receptor Affinity 1 = 2 2 >>> 1 to prostatic hyperplasia (see below). Individual agents may have other important effects in addition to -receptor antagonism (see below). The drug also inhibits reuptake of released norepinephrine by presynaptic adrenergic nerve terminals. Phenoxybenzamine blocks histamine (H1), acetylcholine, and serotonin receptors as well as receptors (see Chapter 16). The pharmacologic actions of phenoxybenzamine are primarily related to antagonism of -receptormediated events. The most significant effect is attenuation of catecholamine-induced vasoconstriction. While phenoxybenzamine causes relatively little fall in blood pressure in normal supine individuals, it reduces blood pressure when sympathetic tone is high, eg, as a result of upright posture or because of reduced blood volume. Cardiac output may be increased because of reflex effects and because of some blockade of presynaptic 2 receptors in cardiac sympathetic nerves. Phenoxybenzamine is absorbed after oral administration, although bioavailability is low; its other pharmacokinetic properties are not well known. The drug is usually given orally, starting with dosages of 10 mg/d and progressively increasing the dose until the desired effect is achieved. A dosage of less than 100 mg/d is usually sufficient to achieve adequate -receptor blockade. The major use of phenoxybenzamine is in the treatment of pheochromocytoma (see below). Most adverse effects of phenoxybenzamine derive from its -receptorblocking action; the most important are orthostatic hypotension and tachycardia. Because phenoxybenzamine is an alkylating agent, it may have other adverse effects that have not yet been characterized. Phentolamine is a potent competitive antagonist at both 1 and 2 receptors (Table 101). Phentolamine reduces peripheral resistance through blockade of 1 receptors and possibly 2 receptors on vascular smooth muscle. Its cardiac stimulation is due to antagonism of presynaptic 2 receptors (leading to enhanced release of norepinephrine from sympathetic nerves) and sympathetic activation from baroreflex mechanisms. Phentolamine also has minor inhibitory effects at serotonin receptors and agonist effects at muscarinic and H1 and H2 histamine receptors. In addition, it is sometimes used to reverse local anesthesia in soft tissue sites; local anesthetics are often given with vasoconstrictors that slow their removal. Unfortunately oral and intravenous formulations of phentolamine are no longer consistently available in the United States. Prazosin is a competitive piperazinyl quinazoline effective in the management of hypertension (see Chapter 11). It is highly selective for 1 receptors and typically 1000-fold less potent at 2 receptors. This may partially explain the relative absence of tachycardia seen with prazosin compared with that of phentolamine and phenoxybenzamine. Prazosin relaxes both arterial and venous vascular smooth muscle, as well as smooth muscle in the prostate, due to blockade of 1 receptors. Prazosin is extensively metabolized in humans; because of metabolic degradation by the liver, only about 50% of the drug is available after oral administration. Terazosin has high bioavailability but is extensively metabolized in the liver, with only a small fraction of unchanged drug excreted in the urine. It differs from prazosin and terazosin in having a longer half-life of about 22 hours. It has moderate bioavailability and is extensively metabolized, with very little parent drug excreted in urine or feces. Tamsulosin is a competitive 1 antagonist with a structure quite different from that of most other 1-receptor blockers. Evidence suggests that tamsulosin has relatively greater potency in inhibiting contraction in prostate smooth muscle versus vascular smooth muscle compared with other 1-selective antagonists. Furthermore, compared with other antagonists, tamsulosin has less effect on standing blood pressure in patients. Recent epidemiologic studies suggest an increased risk of orthostatic hypotension shortly after initiation of treatment. These effects increase the risk of cataract surgery, and complications are more likely in the ensuing 14 days if patients are taking these agents. The patient in the case study at the beginning of this chapter had a left adrenal pheochromocytoma that was identified by imaging. The diagnosis of pheochromocytoma is confirmed on the basis of elevated plasma or urinary levels of norepinephrine, epinephrine, metanephrine, and normetanephrine (see Chapter 6). The major clinical use of phenoxybenzamine is in the management of pheochromocytoma. Patients with this tumor have many symptoms and signs of catecholamine excess, including intermittent or sustained hypertension, headaches, palpitations, and increased sweating. Release of stored catecholamines from pheochromocytomas may occur in response to physical pressure, chemical stimulation, or spontaneously. When it occurs during operative manipulation of pheochromocytoma, the resulting hypertension may be controlled with -receptor blockade or the vasodilator nitroprusside. Nitroprusside is preferred because its effects can be more readily titrated and it has a shorter duration of action. Administration of phenoxybenzamine in the preoperative period helps to control hypertension and tends to reverse chronic changes resulting from excessive catecholamine secretion such as plasma volume contraction, if present. Oral doses of 10 mg/d can be increased at intervals of several days until hypertension is controlled. Some physicians give phenoxybenzamine to patients with pheochromocytoma for 13 weeks before surgery. Other surgeons prefer to operate on patients in the absence of treatment with phenoxybenzamine, counting on modern anesthetic techniques to control blood pressure and heart rate during surgery. Phenoxybenzamine can be very useful in the chronic treatment of inoperable or metastatic pheochromocytoma. Although there is less experience with alternative drugs, hypertension in patients with pheochromocytoma may also respond to reversible 1selective antagonists or to conventional calcium channel antagonists. Beta-receptor antagonists may be required after -receptor blockade has been instituted to reverse the cardiac effects of excessive catecholamines. It has a bioavailability of about 60%, is extensively metabolized, and has an elimination half-life of about 5 hours. Indoramin is another 1selective antagonist that also has efficacy as an antihypertensive. Labetalol and carvedilol have both 1-selective and -antagonistic effects; they are discussed below. Neuroleptic drugs such as chlorpromazine and haloperidol are potent dopamine receptor antagonists but are also antagonists at receptors. Their antagonism of receptors probably contributes to some of their adverse effects, particularly hypotension. Ergot derivatives, eg, ergotamine and dihydroergotamine, cause reversible -receptor blockade, probably via a partial agonist action (see Chapter 16). This increases central sympathetic activation and also promotes increased norepinephrine release in the periphery. It was once widely used to treat male erectile dysfunction but has been superseded by phosphodiesterase-5 inhibitors like sildenafil (see Chapter 12). Yohimbine can greatly elevate blood pressure if administered to patients receiving norepinephrine transport-blocking drugs.
Generic serpina 60 caps buy online. Virtual reality to treat anxiety disorders.
References
- Ang CS, Kelley RK, Choti MA, et al. Clinicopathologic characteristics and survival outcomes of patients with fibrolamellar carcinoma: data from the Fibrolamellar Carcinoma Consortium. Gastrointest Cancer Res 2013;6(1):3-9.
- Hunt GB, Ross DL: Comparison of effects of three anesthetic agents on induction of ventricular tachycardia in a canine model of myocardial infarction, Circulation 78:221, 1988.
- Ordonez NG. Desmoplastic small round cell tumor II: An ultrastructural and immunohistochemical study with emphasis on new immunohistochemical markers. Am J Surg Pathol 1998;22:1314-27.
- Pancherz H. The effect of continuous bite jumping on the dentofacial complex: a follow-up study after Herbst appliance treatment of Class II malocclusions. Eur J Orthod 1981;3: 49-60.
- Ivankovich, A.D., Miletich, D.J., Albrecht, R.F., Heyman, H.J., Bonnet, R.F. Cardiovascular effects of intraperitoneal insufflation with carbon dioxide and nitrous oxide in the dog. Anesthesiology 1975;42:281-287.
- Burstein HJ, Piccart-Gebhart MJ, Perez EA, et al. Choosing the best trastuzumab-based adjuvant chemotherapy regimen: should we abandon anthracyclines? J Clin Oncol 2012;30(18):2179-2182.
- Mazzariol F, Ascher E, et al. Values and limitations of duplex ultrasonography as the sole imaging method of preoperative evaluation for popliteal and infrapopliteal bypasses. Ann Vasc Surg 1999; 13:1.