
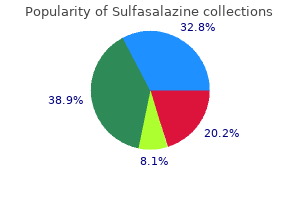
Sulfasalazine
| Contato
Página Inicial
Benjamin D. Solomon, M.D.
- Inova Translational Medicine Institute/Innova Children? Hospital
- Inova Health System
- Falls Church, Virginia
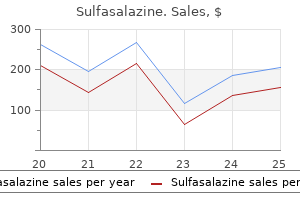
In many patients back pain treatment yahoo order sulfasalazine discount, airway resistance can be overcome by increasing the work of the respiratory muscles pain relief treatment center llc purchase sulfasalazine 500 mg with amex. However pain treatment centers of illinois cheap sulfasalazine 500 mg otc, normal passive expiration may not be enough to promote adequate alveoli emptying unifour pain treatment center statesville cheap sulfasalazine 500 mg buy on-line. Forced expiration generates high intrathoracic pressures that force smaller airways to close nerve pain treatment for shingles buy sulfasalazine 500 mg without a prescription, trapping air in the chest. Investigations the extent of air trapping can be measured using spirometry, which measures the force and volume of a maximum expiration after a full inspiration. An inability to meet a predicted value based on age, sex and height could indicate airway obstruction. Spirometry a normal forced vital capacity compared to an obstructed forced vital a quick and simple assessment of the airways; however, regular peak flow measurements are more revealing than single arbitrary readings and carers should be mindful that peak expiratory flow rates are effort dependent. As a result, airflow becomes obstructed, often resulting in a characteristic wheeze. In extrinsic asthma, airway inflammation is a consequence of hypersensitive reactions associated with allergy, i. Many patients, however, have a combination of both types and, irrespective of causative agents, the physiological changes, symptoms and treatments are the same. Once stimulated, mast cells release a number of cytokines (chemical messengers), which cause physiological changes to the lining of the bronchi and bronchioles. Three such cytokines are histamine, kinins and prostaglandins, which cause smooth muscle contraction, increased mucus production and increased capillary permeability. As the airways become obstructed, the patient finds it increasingly hard to breathe and to cough up the mucus. However, asthma is reversible and it is estimated that 90% of asthma deaths are preventable. The main care goals are: · · · · · Continuous monitoring of vital signs until the patient is stabilised. Safe administration of prescribed bronchodilators and steroids to alleviate dyspnoea (Tables 10. Communication as speaking requires a constant flow of air, patients experiencing acute breathlessness are only able to talk for very short periods before the need to breathe interrupts them. Beta-2 agonists stimulate beta-2 receptor sites in the airways, promoting rapid bronchodilation within 15 minutes, with a duration of 48 hours depending on dose Blocks the action of acetylcholine, a neurotransmitter released by the parasympathetic nervous system. Indication Prophylaxis and reduction of frequency of exacerbations Exacerbation Corticosteroids* Beclametasone Budesonide Fluticasone Prednisolone Hydrocortisone Route Inhaler Care considerations Inhaled corticosteroids can cause hoarseness, loss of voice and candidiasis. Advise patients to rinse their mouths after taking these inhalers Patients taking prednisolone and hydrocortisone will need careful monitoring. They are used to reduce bronchial hyperactivity in patients with asthma, chronic obstructive pulmonary disease and other respiratory diseases where reversibility is present. Health promotion avoidance of triggers, compliance with prescribed pharmacological therapies, smoking cessation and weight reduction in obese patients may reduce the frequency of asthma attacks. The respiratory system and associated disorders Chapter 10 Red flag Life threatening asthma Healthcare professionals should be vigilant when caring for patients with asthma and be able to detect and determine the signs of acute-severe and life-threatening asthma. According to the British Thoracic Society and Scottish Intercollegiate Guidelines Network (2016), if acutesevere asthma is suspected then one or more of the following is present: Peak flow 3350% of predicted or best Dyspnoea accompanied by an inability to complete sentences in one breath Tachypnoea respiratory rate 25 breaths per minute or higher Tachycardia heart rate greater than 110 beats per minute. Chronic asthma sufferers are also at risk of developing fixed airway obstruction as airways become re-modelled over time. Medicines Management Inhaler technique For patients with asthma and chronic obstructive pulmonary disease, it is very important that their inhaler technique is correct. It is estimated that around a third of patients do not use their inhaler correctly, leading to many people receiving lower doses of their prescribed corticosteroids or bronchodilator therapies. Healthcare professionals need to be aware of the Chapter 10 Fundamentals of applied pathophysiology correct techniques for a range of inhalers and be able to advise their patients correctly. Some of the common mistakes made by patients include: Not shaking the inhaler before using them Inhalers contain a propellant that turns the medication into a spray. Not breathing out before inhaling this ensures a deeper and longer inhalation, meaning that more medication enters the airways, increasing its effectiveness. Holding their breath for 10 seconds after inhaling provides more time for the medication to get into the airways, also increasing its effectiveness. Inhaling too early Patients often start to inhale before they press their inhaler. Eventually, the right ventricle becomes enlarged and fails, ultimately leading to peripheral oedema. Emphysema Emphysema is defined as the permanent enlargement of airspaces beyond the terminal bronchiole and the destruction of the alveolar wall. The mechanisms behind this degeneration of tissue are thought to relate to the actions of destructive enzymes called proteases, which are released from neutrophils and macrophages in response to infection. In health, lung tissue produces a substance called alpha antitrypsin, which counteracts the destructive action of protease. Smoking, however, is thought to reduce the effect of alpha antitrypsin and increase protease activity, allowing alveolar destruction to continue unabated (Hogg and Senior, 2002). Proteases destroy the elastic fibres essential for elastic recoil, which is much needed during exhalation. The increased volume of air within the thorax pushes the diaphragm downwards, disturbing its natural concave shape and making breathing difficult. Frequent infections can also develop as it becomes increasingly difficult to cough up secretions. The destruction of the alveolar wall and adjacent capillaries will mean that there is less lung tissue available for external respiration and the patient will be at risk of developing hypoxaemia and hypoxia (Gould, 2006). Chronic bronchitis Chronic bronchitis is defined as the presence of a productive cough lasting for 3 months in each of 2 consecutive years when other pulmonary and cardiac causes of cough have been ruled out (Braman, 2006). This chronic irritation causes inflammation and the bronchial wall thickens, causing airway obstruction. The lack of functioning cilia makes mucus clearance difficult and as a result, mucus collects and blocks the smaller airways. As more and more airways become blocked, external respiration is reduced and less oxygen is transferred into the bloodstream. The pathophysiological processes behind increased mucus production and cilia dysfunction are thought to involve an inflammatory response to the constant bombardment by cigarette smoke (MacNee, 2006). However, wherever possible, the patient should be managed by the multidisciplinary team in their own home. Alison rarely drinks alcohol but has smoked 20 cigarettes a day since she was 16 years old. She is currently unemployed and lives in a small council flat on the outskirts of town. She has recently found that she becomes increasingly breathless on exertion and when she woke up this morning she could not catch her breath. The nurses takes a set of vital signed and a doctor takes an arterial blood sample for gas analysis (see below). The respiratory system and associated disorders Chapter 10 Vital signs On admission to the A&E department the following vital signs were noted and recorded: Vital sign Temperature: Pulse: Respiration: Blood pressure: O2 saturation: Observation 36. Typically a lung function test will incorporate three specific investigations: Spirometry: Spirometry measures the force and volume of a maximum expiration after a full inspiration. However, for a lung function test, patients are placed in a sealed glass booth, with clips on their noses to prevent air escaping and ensuring a more accurate lung volume measurement. A harmless dose of carbon monoxide is inhaled, then blood samples are taken and the level of carbon monoxide present is measured. Therefore patients may need to abstain from bronchodilator therapy before their test. Analgesia may also affect the results, so patients should tell the medical team if they have taken any pain relief prior to the test. Patients should be advised to avoid eating large meals before the test, as a full stomach can impede full inhalation. It is advisable that patients wear loose fitting clothes and avoid wearing jewelry so as to facilitate deep breathing. People who wear dentures should be advised to keep them in to help maintain a seal around the mouth pieces used for inhalation. Being placed in a glass booth can cause feelings of claustrophobia and anxiety and patients will need comfort and reassurance that the procedure is harmless and painless. Bronchiectasis Bronchiectasis describes an irreversible lung condition caused by recurrent infection and inflammation. The condition is associated with abnormal dilation of the bronchi together with a loss of functioning cilia. It is characterised by a chronic productive cough, in which the patient produces large amounts of purulent sputum. Bronchiectasis is a chronic lung disorder that usually develops secondary to a problem during childhood. Inflammation as a result of severe pneumonia, measles or whooping cough during childhood damages and weakens the bronchial walls. Less common are congenital causes such as cystic fibrosis, in which the overproduction of viscous mucus causes recurrent lung infections, and immunoglobulin deficiencies, which cause recurrent infections (Goeminne and Dupont, 2010). Restrictive disorders Patients with restrictive disorders have difficulty in expanding their thorax. This is because the airways are not obstructed, but rather chest expansion is restricted. Poliomyelitis, amyotrophic lateral sclerosis and botulism, for example, can cause respiratory muscle paralysis, whereas muscular dystrophy causes muscle weakness. Disorders that restrict lung tissue are in the main chronic conditions caused by the inhalation of industrial or commercial pollutants. The upper respiratory tract is often unable to the respiratory system and associated disorders Chapter 10 handle the vast quantities of airborne particles generated by various work practices. Over time, connective tissue within the lungs is eroded and the lungs become less compliant, making chest expansion difficult. This group of respiratory diseases is called pneumoconioses and the individual diseases are often named after the job or pastime that generated them. Chest expansion can also be restricted by acute problems such as adult respiratory distress syndrome, which occurs after lung trauma or pulmonary oedema. Lung cancer Lung cancer has the highest mortality rate of all known cancers in the Western world. Also susceptible are those exposed to passive smoking, albeit at a much lower probability. Certain chemicals present within cigarette smoke are carcinogenic, and promote the development of tumours within the lung tissue. The vast majority of lung cancers (95%) are bronchial carcinomas of which there are two major types non-small cell and small cell. Non-small cell carcinomas account for 70% of all lung cancers and can be subdivided again into squamous cell carcinomas, which tend to develop within the larger bronchi, and adencarcinomas and large cell carcinomas, which are found in the smaller airways, making them much harder to detect. Small cell carcinomas tend to grow near a large bronchi and are the most aggressive bronchial carcinomas. Pleural disorders Only a minute amount of fluid occupies the pleural space (the space between the parietal and visceral pleura). The collapse of a lung results in areas that are under-ventilated, a phenomenon known as atelectasis. The surface area for external respiration is dramatically reduced and the patient may develop hypoxaemia (West, 2013). Trauma, cancer and surgery can all cause bleeding into the pleural space, a phenomenon referred to as haemothorax. Exudate and transudate pleural effusions can cause other kinds of fluid to collect in the pleural space. Inflammation increases capillary permeability, allowing fluid to leak out of blood vessels and into the pleural space. A decrease in blood osmotic pressure will also force fluid from blood vessels into the pleural space; causes of reduced blood osmotic pressure include hypoproteinaemia. Some patients may develop an empyema, the formation of pus in the pleural effusion (Dobbin and Howard, 2009). Pleural effusion Dyspnoea Pleuritic pain Dry cough Cyanosis Tachycardia Pneumothorax Tachypnoea Use of accessory muscles Asymmetrical chest expansion Cyanosis Tachycardia Hypertension or hypotension Pulsus paradoxus Sweating Dry cough Restlessness or confusion the respiratory system and associated disorders Chapter 10 respiratory disease are also at risk of developing a pneumothorax. Some individuals have a congenital defect or bleb within the alveolar wall which can rupture spontaneously. In certain circumstances, a flap of tissue creates a one-way valve effect and airflow into the pleural space is promoted with each inspiration. As the pneumothorax grows, pressure is exerted on the inferior vena cava, impeding the blood flowing back to the heart (venous return). Care and management Chest drains are often used to assist the re-inflation of the affected lung. The monitoring of both the patient and the drain is the responsibility of the healthcare professional and attention should be paid to the following: · · · · 305 · · · Patient positioning placing the patient in an upright position will encourage drainage and aid expansion of the thorax. Coiled and looped tubing should also be avoided as it can impede drainage flow and lead to a tension pneumothorax or surgical emphysema. Close monitoring of the chest drain: · Swinging the level of the fluid in the underwater seal of the drain should fluctuate between 5 and 10 cm when the patient breathes. Accurate recording of drainage the quantity, colour and consistency of the fluid being drained should be noted. Infection control the insertion site should be checked daily for signs of infection, i. Conclusion this chapter has examined how respiratory disorders can interfere with respiration. Respiration involves four distinct physiological processes: pulmonary ventilation, external respiration, transport of gases and internal respiration.
Superior vena cava the large vein that returns oxygen-depleted blood superior to the diaphragm to the right atrium pain disorder treatment plan discount 500 mg sulfasalazine otc. Systemic circulation the flow of blood from the left ventricle to all parts of the body ocean view pain treatment center order sulfasalazine cheap. National Clinical Guidelines for diagnosis and management in primary and secondary care milwaukee pain treatment center milwaukee wi sulfasalazine 500 mg order without a prescription. As the blood flows through the arterial system groin pain treatment exercises 500 mg sulfasalazine with amex, it transports nutrients and other substances essential for cellular metabolism and for homeostatic regulation pain treatment alternative discount sulfasalazine 500 mg. The waste products of metabolism are transported by the venous system for removal by the kidneys, lungs and skin. This chapter discusses the structure and functions of the blood vessels, factors affecting blood pressure, and vascular disorders and their related care. Overview of blood vessels In the human body there are several kinds of blood vessels. They transport oxygen-rich (oxygenated) blood, except the pulmonary artery which carries oxygen-depleted blood. Veins and venules carry blood towards the heart and transport oxygen-depleted (deoxygenated) blood, except the pulmonary veins which carry oxygenated blood. Capillaries are the minute blood vessels where arteries terminate and veins begin. They form a delicate network of vessels and are in close proximity to most parts of the body tissues. Blood vessels can dilate, constrict, pulsate and form a closed delivery system for the blood which begins and ends at the heart. The outer layer is called the tunica externa, formally known as the tunica adventitia. It is largely composed of collagen fibres that protect and support the blood vessels, and secure them to the surrounding tissues. The tunica externa is supplied with sympathetic nerve fibres and lymphatic vessels; the larger veins are also supplied with elastic fibres (Jenkins and Tortora, 2013). The tunica media is the middle layer and it contains smooth muscles and elastic tissue. As the blood vessels constrict or dilate the blood pressure increases or decreases, respectively. This lining makes the inner surface smooth, thus minimising friction as the blood flows through the vessel. Although the role of the blood vessels is to transport blood, the tunica externa of the large blood vessels receives its blood supply via a network of blood vessels called the vasa vasorum. Vessels with thin walls receive oxygen and nutrients by diffusion from the blood passing through the lumen. Arteries Arteries can be subdivided into three groups elastic arteries, muscular arteries and arterioles. Elastic arteries are thick-walled vessels found near the heart of which the aorta is the main artery. This ensures that the blood is moving forward, even though the left ventricle is relaxed. As these arteries conduct blood from the left ventricle to the small arteries, they are sometimes referred to as conducting arteries. From the elastic arteries the blood flows into the medium-sized arteries, called the muscular arteries. They contain more smooth muscles and fewer elastic fibres; therefore, they are capable of greater vasoconstriction and vasodilatation. Muscular arteries are also called distributing arteries because they distribute blood to specific organs and parts of the body. They include axilliary, brachial, radial, splenic, femoral, popliteal and tibial arteries. The muscular arteries then divide into smaller arteries called the arterioles and they play an important role in determining the amount of blood flowing into organs and tissues. Larger arterioles have all the three layers, but the tunica media mainly consists of smooth muscle with a few elastic fibres, whilst the arterioles near the capillary end are composed of endothelial cells and an incomplete layer of smooth muscle (Jenkins and Tortora, 2013). When they constrict, blood flow is diverted from the organs or tissue they supply. The thin walls of the capillaries allow water, nutrients, gases and waste products of metabolism to move in and out of the blood and to nearby cells (Jenkins and Tortora, 2013). Capillaries are composed of a single layer of tunica intima and they are found throughout the body, except the epidermis of the skin and the cornea of the eye. The smallest venules are mainly composed of endothelium and a few fibroblast cells. The venules are extremely porous and therefore will allow substance such as water, solutes and white blood cells to move in and out of the vessel into the extracellular fluid. Veins Venules unite to form veins and they contain the same three layers as the arteries. The walls of the veins, compared to the arteries, are thinner and contain less elastic and collagenous tissue and smooth muscle. Like arteries, veins receive their nourishment from tiny blood vessels called vasa vasorum (McCance et al. The blood pressure is low when the person is sleeping at night and increases as the person wakes in the morning. The baroreceptors are located in the carotid sinus and the aortic arch, and they are sensitive to arterial blood pressure changes. These bodies detect changes in oxygen, carbon dioxide and hydrogen ion concentrations. Factors that can affect blood pressure Several factors affect blood pressure and they include: · · · · · cardiac output circulating volume peripheral resistance blood viscosity hydrostatic pressure. Diseases of the blood vessels On completion of this section the reader will be able to: · · · · List some of the common diseases of the blood vessels and the risk factors associated with these diseases. Describe the pathophysiological responses associated with specific vascular health problems. Outline the care and management and interventions related to the disorders described. Case study Mrs Carly Symmons is a 66-year-old widow who lives in a first-floor flat. She is overweight and smokes approximately 30 cigarettes per day but does not drink any alcohol. Mrs Symmons has a small ulcer on her left ankle, which she cared for herself, but lately has noticed that the ulcer is weeping and she had pains in her left leg. Vital signs the practice nurse notes and records the following vital signs: Vital sign Temperature: Pulse: Respiration: Blood pressure: O2 saturation: Observation 38. Discuss the health education/promotion advice that you will give Mrs Symmons before she is discharged from hospital. Atherosclerosis/arteriosclerosis Arteriosclerosis is the term describing arterial disorders in which degenerative changes result in decreased blood flow. Atherosclerosis is the most common form of arteriosclerosis where there is thickening and hardening of the vessel walls due to lipid accumulation. This condition is found mainly in the large- and medium-sized arteries, such as the aorta and its branches, the coronary arteries and the arteries that supply the brain, whereas arteriosclerosis mainly affects arterioles (Nowak and Handford, 2010). Aetiology the cause of atherosclerosis is not known, but certain risk factors have been identified: · · · · · · · · · hypertension cigarette smoking (nicotine has a vasoconstricting effect) high lipid levels in the blood familial history obesity diabetes mellitus (high serum glucose levels cause vascular damage) lifestyle alcohol gender (men are at a higher risk than women). The vascular system and associated disorders Chapter 7 Investigations the following investigations may be carried out confirm diagnosis: · · · · full blood chemistry Doppler ultrasound electrocardiogram arteriogram. Nurses must adhere to their local policies in the preparation and in the safe management of patients undergoing arteriogram, and offer physical and psychological support. A needle is then inserted into the artery, and a long fine tube (catheter) is placed in position. The special dye (contrast medium) is then injected through the catheter and X-rays taken. Once the radiologist is satisfied with the X-rays, the catheter will be removed and the radiologist will press firmly on the skin over the entry site for 10 minutes until the artery stops bleeding. Post procedure, the nurses must adhere to local policy and procedure in caring and management of patients who have undergone arteriogram. Regular inspection of the puncture site is important to ensure that there are no complications such as secondary bleeding, excess pain the groin area and haematoma. Nurses must report to the nurse in charge immediately, if they observe any of these signs, so that prompt action can be taken. Every precaution should be taken to ensure that evidence practice is carried out following arteriogram investigation. Pathophysiology of atherosclerosis Atherosclerosis is a form of arteriosclerosis where the walls of the arteries are hard, thick and narrow as a result of lipid accumulation within the arterial walls. Greater blood pressure is needed to push the blood through these narrow blood vessels, which leads to hypertension. Although atherosclerosis can affect any organ or tissue, the arteries supplying the heart, brain, small intestines, kidneys and lower extremities are mostly affected. Signs and symptoms of atherosclerosis · · · · diminished or absent pulses skin is pallor or cyanosed pain muscle weakness. Site Abdominal aorta Effects Gangrene of toes and feet Aneurysms Intermittent claudication Gangrene of toes and feet Aneurysms of iliac arteries Angina pectoris Myocardial infarction Transient ischaemic attack Cerebrovascular accident Hypertension, renal ischaemia Intestinal ischaemia Aorto-iliac and femoral arteries Coronary arteries Carotid and vertebral arteries Renal arteries Mesenteric arteries the vascular system and associated disorders Chapter 7 Care and management A full care history is essential in order to provide high-quality care for patients with atherosclerosis. The assessment must include the identification of risk factors and symptoms of any cardiovascular disease. The care and management includes: · · · · Health promotion to prevent the disease must include advice on a healthy diet and regulating the lipid levels within normal range. Advice on the cessation of smoking and alcohol consumption should be offered as these are identified risk factors in atherosclerosis. Patients should be advised to lose weight if obesity is a problem Encourage the patient to undertake programmed exercise under the supervision of healthcare professionals. This will help in lowering their weight and cholesterol level, and in reducing their blood pressure and stress. The medications include: · · · · antihypertensives such as beta-blockers anticoagulant therapy with heparin lipid-lowering drugs such as simvastatin antiplatelet drugs. In some patients, surgical procedures, such as balloon angioplasty, may be indicated to improve the blood flow through the vessel. Statin therapy is recommended for adults at high risk of cardiovascular disease (heart attack, stroke or peripheral artery disease) and also those who already have a history of cardiovascular disease. They do this by blocking the synthesis of cholesterol in the liver cells; the cells then get their supply of cholesterol from the blood, thereby lowering the blood cholesterol level. Some side effects have been documented with this medication including headache, stomach upset, altered liver function and some muscle pain but these side effects are usually mild, easily recognisable and reversible. It is essential to note that many people will have no side effects at all from this medication. Hypertension Hypertension refers to sustained elevation in systemic arterial blood pressure (McCance et al. There are many classifications of Chapter 7 Fundamentals of applied pathophysiology hypertension, some of which are based on severity. Secondary hypertension where there is an underlying cause, such as renal diseases or tumour of the adrenal medulla. Malignant hypertension occurs in the younger age groups with renal and collagen diseases. Isolated systolic hypertension mainly occurs when a combination of factors is seen in the elderly, and is due to increases in cardiac output, increased peripheral resistance and renal vascular resistance. Aetiology Although the cause or causes of primary hypertension is unknown, several risk factors have been identified for its development: · · · · · · · · · · · obesity stress cigarette smoking and alcohol consumption excessive intake of sodium causing fluid retention family history. The vascular system and associated disorders Chapter 7 Investigations these include: · · · · full blood chemistry physical examination electrocardiogram assessment of risk factors. Common presenting symptoms Many patients are unaware that they have hypertension and go untreated. It is frequently identified through blood pressure screening or as a result of other diseases. Some patients have reported blurred vision and tinnitus, but usually when symptoms of hypertension do occur, the disease is at an advanced stage (Bullock and Henze, 2010). In most cases, the focus is on kidney diseases or excessive levels of hormones such as aldosterone and cortisol. These hormones stimulate the retention of sodium and water, resulting in increased blood volume and blood pressure. Once the underlying cause is treated, such as with the removal of the diseased organ, the blood pressure returns to normal. Malignant hypertension this is a rapidly progressive hypertension where the diastolic pressure is in excess of 120 mmHg (Waugh and Grant, 2014), which can result in encephalopathy, cerebral oedema and loss of consciousness. Malignant hypertension does not indicate that there is cellular injury, but because it is life-threatening, it is considered as an emergency. If untreated, cerebral oedema and cerebral dysfunction occur, leading to death of the individual. In isolated systolic hypertension, the systolic blood pressure is over 140 mmHg and the diastolic pressure is less than 90 mmHg (Hogan et al. It is recognised as an important risk factor for cerebrovascular accident and cardiac failure, and thus should be treated as a medical emergency. Chapter 7 Fundamentals of applied pathophysiology Non-pharmacological interventions · · 192 · · · · A single recording of raised blood pressure does not indicate that the patient is suffering from hypertension.
Healthcare professionals need to recognise various signs and symptoms quickly and take immediate action to prevent any further complications arising from the illness neck pain treatment+videos purchase sulfasalazine with paypal. Ongoing assessment and evaluation of interventions are important in order to respond to the changing needs of the patient low back pain treatment guidelines purchase sulfasalazine, which may have implications for patient outcomes pain treatment center of the bluegrass ky buy 500 mg sulfasalazine otc. The walls and lining of the pericardial cavity are a special membrane known as the pain treatment ovarian cyst 500 mg sulfasalazine buy with visa. Pericardium is a type of that produces to lubricate the heart and prevent friction between the ever beating heart and its surrounding organs pain treatment center richmond ky buy sulfasalazine uk. Besides lubrication, the pericardium serves to hold the heart in and maintain a hollow space for the heart to expand into when it is full. The pericardium has layers-a that covers the outside of the heart and a that forms a around the outside of the pericardial cavity. The is the outermost layer of the heart wall and is just another name for the of the pericardium. The is the muscular middle layer of the heart Chapter 6 Fundamentals of applied pathophysiology wall that contains the. The endocardium is very smooth and is responsible for keeping blood from sticking to the inside of the heart and forming. Apex; Base; Blood clots; Cardiac muscle tissue; Endocardium; Epicardium; Lung; Myocardium, Pericardial cavity; Parietal layer; Pericardium; Position; Sac; Serous fluid; Serous membrane; Squamous endothelium; Sternum; Thoracic cavity; Two; Visceral layer 172 Label the diagram From the list of words supplied, label the diagram. A protein that is the main organic component of connective tissues the heart and associated disorders Chapter 6 Further resources Online nutritional information and facts. This website discusses dietary and medical misinformation on congestive heart failure. This site discusses heart failure, symptoms, causes, diagnosis, treatment and prevention. This site discusses angina, symptoms, causes, diagnosis, treatment and prevention. Antidiuretic hormone a protein hormone produced in the hypothalamus and stored in the posterior pituitary gland; it aids reabsorption of water by the kidneys. Atherosclerosis a condition where cholesterol and lipid deposits accumulate on the inner layer of the medium and large blood vessels, leading to narrowing of these vessels. Athromatous plaque a collection of lipids and cholesterol that accumulates in large- and medium-sized vessels. Atrioventricular valve a heart valve made up of membranous flaps that allow blood to flow in one direction only; also known as the bicuspid valve. Chapter 6 Fundamentals of applied pathophysiology 176 Bicuspid valve as its name suggests, it contains two cusps; also known as the atrioventricular valve. Inferior vena cava the large vein that returns oxygen-depleted blood from all parts of the body below the diaphragm to the right atrium. Medulla oblongata the lowest portion of the brain; concerned with the control of internal organs. Myocardial infarction death of an area of heart muscle due to an interruption of the blood supply to the affected area. Pulmonary artery the vessel that takes oxygen-depleted blood from the right ventricle to the lungs. Pulmonary oedema the abnormal collection of fluid in the tissue space and the alveolar sac. Pulmonary vein the vessel that returns oxygenated blood from the lungs to the left atrium. Semilunar valve a valve that prevents the backflow of blood to the ventricles after contraction. At least three recordings of raised blood pressure at different intervals are required to confirm hypertension. This measurement is much more accurate than the blood pressure measurements done in the clinic. Advise the patient to restrict sodium intake as sodium promotes water retention, resulting in increased circulating volume and increased cardiac output, which lead to hypertension. Healthcare professionals need to advise the patient on the cessation of cigarette smoking and excessive alcohol consumption. A diet rich in fruit and vegetables and low in saturated fats can help in the reduction of blood pressure. Reduction of salt in cooking should be encouraged as excessive intake of salt promotes fluid retention, thus increasing circulating volume. Encourage patients to reduce their stress levels because relaxation aids in the reduction of blood pressure by decreasing the workload of the heart. Listening to music, gardening and going for walks have all been identified as helpful in the reduction of blood pressure. Pharmacological interventions In some patients, non-pharmacological interventions are sufficient in controlling their blood pressure, while in others combinations of both pharmacological and non-pharmacological methods are used in the treatment of hypertension. The medications include: · · Diuretics are prescribed to reduce fluid load, which leads to reduction in cardiac output, thus helping to reduce blood pressure. If the doctor recommends it, you could prevent potassium loss by taking a liquid or tablet that has potassium along with the diuretic. People with diabetes may find that diuretic drugs increase their blood sugar level. A change in medication, diet, insulin or oral anti-diabetic dosage corrects this in most cases. Aneurysm An aneurysm is a permanent dilatation of an artery or a chamber of the heart. Although it can occur in both arteries and veins, the aorta and the arteries at the base of the brain are the vessels most susceptible to aneurysms. It can occur in a localised part of the aorta or all along the vessel (Brooker et al. The commonest cause of an aneurysm is atherosclerosis because the fatty deposits erode and weaken the vessel wall. Damage to the structure of the arteries creates weaknesses that can lead to brain aneurysms Aetiology There are several causes and they include: · · · · Atherosclerosis main cause of an aneurysm affecting the descending aorta. Hypertension due to constant pressure, weakening of the vessel wall can occur in the elderly. Investigations these include: · · full blood chemistry angiography Chapter 7 Fundamentals of applied pathophysiology · · ultrasound chest X-ray. Symptoms Most aortic aneurysms are asymptomatic until they start to leak or rupture and the symptoms vary depending on the affected vessel. Symptoms may include: 194 · · · · pain in the abdominal region or in the extremities due to compression of neighbouring organs dyspnoea (shortness of breath or difficulty in breathing) due to pressure on internal organs dysphagia (difficulty in swallowing) signs and symptoms of cerebrovascular accident occur if the cerebral arteries are affected. Care and management the main treatment for an aneurysm is surgery, and therefore it is vital that a full assessment of the patient is obtained. All care given should be documented in accordance with local policy and procedure and adherence to the Nursing and Midwifery Council Code (2015). The vascular system and associated disorders Chapter 7 Pharmacological interventions the following medications may be prescribed for a patient with an aneurysm: · · · · antihypertensives anticoagulants antibiotics analgesics. Mr Lee smokes 40 cigarettes per day and drinks two cans of lager every day after work. Lately his right leg has been aching so much that he has to stop during his delivery rounds to ease the pain and to catch his breath. Investigations these include: · · · · · Doppler ultrasound arteriogram/venogram full blood chemistry physical examination electrocardiogram. The vascular system and associated disorders Chapter 7 Clinical investigations Doppler ultrasound the test involves measuring the blood pressure in the ankles and comparing it to the blood pressure in the upper arms. These measurements are taken with a Doppler probe, which uses sound waves to determine the flow of blood in the arteries. However, in peripheral arterial disease, the blood pressure in the ankles will be lower than that in the arms. A more severe blockage can lead to the development of gangrene, usually in the toe (Stubbling and Chesworth, 2010). Venous insufficiency may occur as the result of an obstruction in the veins by a thrombus or incompetent valves, which can lead to the formation of a venous ulcer as a result of poor circulation. There are distinct differences between arterial and venous insufficiency (Table 7. Signs and symptoms · · · · · · intermittent claudication white, pale colour when legs are elevated leg ulcers (Table 7. Arterial Pain Sudden severe pain, rest pain, intermittent claudication Diminished or absent Mainly in the toes, feet or other areas of the skin Shiny, cool or cold temperature; mild oedema if present Gangrene Doppler pressure readings lower below blockage Venous Aching and cramp relieved by elevating the foot Present Mainly over the inner or outer ankle Pulse Ulcer characteristics Skin characteristics Thick and tough; skin normal colour; may have oedema, warm to touch Poor healing Normal pressure reading Complications Blood flow Chapter 7 Fundamentals of applied pathophysiology Care and management Pain control is paramount in patients with arterial insufficiency. If pain is caused by exercise, such as walking long distances, then the patient should be advised against it. However, light exercise that can be tolerated should be encouraged as it helps to improve circulation. Patients should be advised to keep themselves warm if they are affected by cold weather, but they should avoid the following: 198 · · · · · · Tight fitting clothing as this restricts arterial blood flow. Hot baths or sitting near fires because of the risk of burns with decreased sensation to the limbs Cutting toenails as soft tissue damage may be slow to heal because of poor peripheral circulation. Sitting cross-legged for too long as this will restrict blood flow to the lower limbs. A well-balanced healthy diet high in fruit, fibre and vegetables and low in saturated fat should be encouraged. Postoperative complications should be reported and treated immediately to prevent undue harm to the patient. Aspirin is available as a generic drug, and is prescribed for treating fever, pain, inflammation in the body, prevention of blood clots, and reduction of the risk of strokes and heart attacks. Aspirin is an antiplatelet medicine, which means it reduces the risk of clots forming in the blood. Normally, when there is a cut or break in a small blood vessel, a blood clot forms to plug the hole until the blood vessel heals. Some of the serious side effects include: · black, bloody, or tarry stools; · coughing up blood or vomit that looks like coffee grounds; · severe nausea, vomiting, or stomach pain; · fever lasting longer than 3 days; · swelling, or pain lasting longer than 10 days 199 Venous insufficiency/varicose veins Varicose veins are vessels that have become dilated and tortuous due to incompetent valves, which allow back flow and pooling of blood in the veins. People who are susceptible to varicose veins are pregnant women, the obese, those who have to stand for long periods because of the nature of their occupation. Signs and symptoms swelling of the lower extremities distended and tortuous veins dull aching in the leg ulcers (rare) leg fatigue and heaviness. Postoperative care includes applying pressure bandages for about 6 weeks, elevating the foot and gradually increasing ambulation (LeMone et al. The surgical treatment is successful; however, 2030% of the patients may require repeat surgery. Pain should be managed by bed rest and elevation of the feet, which improves venous return. Supportive anti-embolism stockings should be worn to reduce swelling in the leg and to provide support to the veins. Encourage adequate fluid intake of 23 L per day and a healthy diet for tissue healing. Hypercoagulability of blood due to dehydration, hormone replacement therapy and oral contraceptive pills. Use of intravenous cannulae may cause damage to the tunica intima, resulting in the formation of clots. Other factors include age (people over the age of 40 years are at greater risk), obesity, pregnancy, varicose veins and smoking. Pathophysiology A thrombus can develop in the superficial or deep veins of the legs. The blood flow is sluggish in the affected vessels and the clotting cascade takes place. Platelets aggregate at the site of injury to the vessel wall or where there is venous stasis (LeMone et al. Platelet aggregation occurs because platelets are exposed to collagen (a protein in the connective tissue, which is found in the inner surface of the blood vessel). When platelets come into contact with the exposed collagen, they release adenosine diphosphate and thromboxane. The thrombus triggers the inflammatory response, causing tenderness, swelling and erythema at the affected site. Initially the thrombus stays within the affected area; however, fragments of the thrombus may become loose and travel through the circulation as an embolus, which may lodge in the lungs and cause a pulmonary embolism. Red flag A blood clot (thrombus) in the deep venous system of the leg is not dangerous in itself. The situation becomes life-threatening when a piece of the blood clot breaks off (embolus, pleural = emboli), travels downstream through the heart into the pulmonary circulation system, and becomes lodged in the lung. Care and management Maintain the patient on bed rest until mobilisation is encouraged. Monitor the vital signs (temperature, pulse, respiration and blood pressure) of the patient 12 hourly to prevent complications such as pulmonary embolism. The vascular system and associated disorders Chapter 7 · · · · · · · Observe the calf muscle for swelling. Measurements should be accurately recorded as changes will allow prompt interventions. The patient should be advised not to massage the affected calf muscle so as not to dislodge the clot. Check every 4 hours if the patient is experiencing any pain or discomfort in the affected leg. Conclusion the overall aim of this chapter was to provide the reader with an understanding of the vascular system and its related disorders. In order to care for the patient with vascular dysfunction, healthcare professionals need to understand the normal physiology of the vascular system. There are numerous diseases related to the vascular system; however, it is not the remit of this chapter to cover all of them. Caring for patients with vascular disorders requires skilled management, which incorporates ongoing assessment, and implementing and evaluating the care.
Thus wrist pain yoga treatment trusted 500 mg sulfasalazine, to allow precision dosing in the practice of anesthesiology gallbladder pain treatment home remedies buy 500 mg sulfasalazine visa, these complex calculations should ideally be incorporated into drug-specific infusion pumps pain treatment hepatitis c 500 mg sulfasalazine order amex. The therapeutic threshold of a drug depends on the magnitude of the desired effect or the intensity of the stimulus being treated blaustein pain treatment center order sulfasalazine with visa. Therefore pain treatment dementia buy generic sulfasalazine on-line, the dose of fentanyl that produces analgesia for superficial procedures (black solid concentration profile) does not produce clinically discernible analgesia for the orthopedic procedures. In contrast, the dose of fentanyl that produces analgesia for the orthopedic procedures (blue solid concentration profile) will not only provide analgesia for the superficial procedures, but it will also have a faster onset of effect because it reaches the therapeutic threshold quicker. In addition, since the larger bolus of fentanyl results in concentrations of drug that are above the toxic threshold for the superficial procedures (red dashed line, Low Toxic Threshold), the patient will have significant ventilatory depression until the effect site concentration of fentanyl decreases below this toxic threshold. This profound ventilatory depression would start approximately 2 minutes after the larger bolus of fentanyl was administered and last until 18 minutes after the larger bolus of fentanyl. The therapeutic window that should be targeted to provide adequate analgesia after a superficial procedure is below the toxic threshold (red dashed line) and above the therapeutic threshold (green dashed line). The therapeutic window that should be targeted for orthopedic 691 procedures has the entire window "shifted higher". Representative therapeutic thresholds (the minimum concentration required to produce clinically discernible analgesia), and toxic threshold (the concentration above which profound opioid induced ventilatory depression occurs) are demonstrated superficial procedures, such as mastectomy (green dashed line, low therapeutic threshold), and for orthopedic procedures, such as long bone instrumentation (dotted green line, high therapeutic threshold). A given bolus of fentanyl only produces clinically discernible analgesia from the time it produces an effect site concentration above the therapeutic threshold concentration for a patient until the time when the effect site concentration decreases below the therapeutic threshold concentration. If the effect site concentration does not exceed the toxic threshold for a patient, then it does not produce profound opioid induced ventilatory depression. In contrast, if the bolus does produce an effect site concentration above the toxic threshold concentration, it will produce profound ventilatory depression that is sustained until the effect site concentration decreases below the toxic threshold concentration. For example, after superficial surgery, a small dose of fentanyl (solid black line) will initially produce detectable analgesia approximately 2 minutes after administration (when it crosses the low therapeutic threshold, dashed green line) which will last until approximately 10 minutes after administration (when the concentration decreases below the low therapeutic threshold, green dashed line). Since the dose does not produce a concentration above the low toxic threshold (dashed red line), hypoventilation will not occur after this single bolus. In contrast, for the same superficial procedure, a larger bolus of fentanyl (solid blue line) will initially produce analgesia less than 1 minute after administration (when it crosses the low therapeutic threshold, dashed green line), which will last until approximately 30 minutes after administration (when the concentration decreases below the low therapeutic threshold, green dashed line). Since the dose produces an effect site concentration above the toxic threshold (dashed red line), it will produce profound 692 hypoventilation from approximately 2 minutes until the effect site concentration decreases below the same toxic threshold at approximately 18 minutes. So, although the larger bolus produces a quicker onset of action and a longer duration of action, it produces toxicity for a portion of this time. After orthopedic procedures (dotted green line for high therapeutic threshold and dotted red line for high toxic threshold), a small bolus of fentanyl will be subtherapeutic and ineffective (black solid line) because it does not produce a concentration above the high therapeutic threshold (dotted green line). In contrast, a larger bolus of fentanyl produces clinically discernible analgesia from approximately 2 through 10 minutes after administration (time that blue line is above green dotted line). Consequently, thorough understanding of the mechanisms of drug interactions and knowledge of specific interactions with drugs used in anesthesia are essential to the safe practice of anesthesiology. For example, moderate to high doses of opioid are often utilized to decrease the amount of volatile anesthetic required to provide immobility and hemodynamic stability to surgical incision. In this section, we will examine the major classes of drugdrug interactions by detailing common examples encountered in the perioperative period. Pharmaceutical (Physiochemical) Interactions In Vitro Interactions Anesthesiologists often overlook the drug interactions produced by pharmaceutical (physicochemical) properties because most perioperative drugs are administered intravenously or via inhalation, and therefore have a high bioavailability. However, in vitro drugdrug interactions due to physiochemical properties of drugs can significantly alter drug bioavailability and produce unintended toxic byproducts. Although physiochemical drug interactions that affect the bioavailability of drugs are relatively easy to avoid or, at least, overcome by increasing the drug dose, some physiochemical interactions can result in unintended toxic compounds. One chemical agent often overlooked by anesthesiologists is the soda lime or Baralyme that is used in modern anesthesia machines to remove carbon dioxide from the exhaled gases. Although patients are not directly administered this agent, the gas that they inhale from the anesthesia machine often contains the byproducts of the interaction between the constituents of the exhaled gas and the carbon dioxide absorbent. While this allows the patient to receive a "heated and humidified" inhaled gas mixture, if conditions are correct, the halogenated volatile anesthetics can undergo degradation by the strong base. The first approach, which was approved for use in the European Union in 2008 and in the United States in 2016, is the selective relaxant binding agent, sugammadex. Sugammadex is a synthetic cyclodextrin that encapsulates and electrostatically binds rocuronium. By essentially irreversibly binding plasma rocuronium, sugammadex acts as a chelator that not only rapidly decreases the free plasma rocuronium concentration but also promotes redistribution of rocuronium from the neuromuscular junction (extracellular space) to the intravascular space. Although sugammadex was developed to antagonize neuromuscular blockade produced by rocuronium, it is also able to antagonize profound neuromuscular blockade produced by the other commonly used steroidal neuromuscular blocking agents, vecuronium and pipecuronium. However, molecules from the cucurbit[n]uril family can encapsulate both the steroidal and benzylisoquinoline family of neuromuscular blocking agents in preclinical models and may be a more comprehensive solution for antagonism of neuromuscular blockade via molecular encapsulation. This approach has led to Phase 1 studies of a new class of nondepolarizing neuromuscular blocking drugs called the fumarates (olefinic diester isoquinolinium compounds). These molecules are rapidly inactivated by the nonenzymatic formation of cysteine adducts when combined with plasma cysteine. These two novel approaches to drug development could be used to develop designer drugs that can be readily antagonized via nonbiologic routes, if the important receptor targets for sedation and amnesia components of general anesthesia are identified. Understanding the basis for alterations in the pharmacokinetics allows anesthesiologists to not only avoid unintentional supratherapeutic or subtherapeutic concentrations of the perioperative medications, but also to strategically employ alterations in pharmacokinetics to achieve the desired concentration profile. Absorption (Uptake) 695 Some drugs can alter the absorption of other drugs, by either altering the delivery of drug to site of drug absorption (uptake) or by altering the local blood flow to the site of drug administration. Although this type of drugdrug interaction will alter bioavailability, it should not alter any other pharmacokinetic parameter. Vasoconstrictors that decrease local blood flow and decrease systemic uptake of drug can be beneficial when added to local anesthetic solutions because they prolong the duration of action of the local anesthetic at the site of injection and can decrease the risk of systemic toxicity from rapid absorption. However, when systemically administered, vasoactive drugs can decrease blood flow to skin and muscle, and decrease the systemic uptake of drugs given by subcutaneous or intramuscular injection. In a similar manner, vasoactive agents can alter the ventilationperfusion ratio, thereby altering pulmonary uptake of volatile anesthetics, despite a constant inspired concentration. It can also alter one or all of the intercompartmental clearance parameters of a multicompartmental pharmacokinetic model. There are two main mechanisms purported in textbooks and the clinical pharmacology literature by which drugdrug interactions alter drug distribution-(a) changing the volume of tissue available for drug uptake and (b) changing the amount of drug available for tissue uptake. Since the drug dose required to achieve a desired drug concentration is intimately linked to systemic drug distribution, understanding what common drugdrug interactions produce real alterations in drug distribution can avoid unintentional exposure to subtherapeutic and supratherapeutic drug concentrations. Therefore, drug-induced alterations of cardiac output and the distribution of cardiac output to tissues can change the distribution clearance of other drugs. Once again, vasoactive agents can alter tissue distribution by altering regional blood flow even if the total cardiac output is unchanged. Because the change in the plasma drug concentration produced by a prescribed dosing regimen is 696 inversely related to the distribution clearance, the drug dose must be decreased when vasoactive drugs decrease cardiac output or the distribution of cardiac output; otherwise the patient will be exposed to supratherapeutic drug concentrations. When examining specific pharmacokinetic parameters, an increase in the fraction of unbound drug in the plasma could theoretically increase the total apparent volume of distribution (Vss), as more molecules of drug are available for distribution into the tissue. Although most changes in protein binding will not influence clinical drug exposure, analysis of the equations governing the steady-state pharmacokinetics suggests that drugs that are extensively protein bound, have a high hepatic extraction ratio, and have a low therapeutic index may be the exception that require dose adjustment. First, the number of unoccupied binding sites is several orders of magnitude higher than the number of molecules of anesthetic drug administered in clinical practice. Therefore, it is hard to envision a scenario where a significant amount of displacement could occur. Even if a drug could displace a significant amount of another drug from its protein-binding site, the liver has the capacity available to metabolize this sudden influx of free drug, thereby returning the free drug concentration to the predisplacement concentrations. Finally, the theoretical argument supporting the importance of protein binding on highly lipophilic drugs ignores the fact that lipophilic drugs not only have flow-limited elimination clearance, but also flow-limited tissue distribution. Therefore, the equations supporting the negligible role of protein binding on flow-limited elimination clearance also generalize to include flow-limited tissue distribution. While it may be possible to safely administer opioids in the presence of protease inhibitors such as ritonavir, because opioids can be titrated in small doses to clinical effect, it is more difficult to titrate warfarin or glyburide when instituting short-term antifungal therapy. Therefore, other opioids may have less variability in opioid doseresponse and be better choices than these prodrugs. Cholinesterase inhibitors indirectly antagonize the effects of neuromuscular blockers by increasing the amount of acetylcholine, which displaces the blocking drug from nicotinic receptors. Pharmacodynamic interactions can also occur if two drugs affect a physiologic system at different sites. Hypnotics and opioids, each acting on their own specific receptors, appear to interact synergistically. However, excessive intrasynaptic serotonin levels from decreased reuptake of serotonin have been associated with other antidepressant medications, including serotonin reuptake inhibitors and serotonin norepinephrine reuptake inhibitors (Table 11-6). Therefore, when adequate washout cannot be obtained and methylene blue must be administered, the serotonergic drug should be stopped and not reinstated for 24 hours after the last dose of methylene blue. This is especially important in the perioperative period when other more common clinical states, such as postoperative delirium or perioperative fever, can be associated with the common symptoms of serotonin toxicity, thereby delaying diagnosis. Although cyproheptadine, a serotonin receptor antagonist, is the most common treatment for moderate to severe serotonin toxicity, it is only available as an oral formulation, thereby limiting its bioavailability in critically ill perioperative patients. Intravenous chlorpromazine is an alternative serotonin receptor antagonist that has been used successfully with concomitant supportive care. Anesthesiologists have become accustomed to the exquisite control of anesthetic blood (and effect site) concentrations afforded by modern volatile anesthetic agents and their vaporizers, coupled to end-tidal anesthetic gas monitoring. In most pharmacotherapeutic scenarios outside of anesthesia care, the time scales for onset of drug effect, its maintenance, and its offset are measured in days, weeks, or even years. This is particularly true of lipid-soluble hypnotics and opioids that rapidly and extensively distribute throughout the various tissues of the body, because distribution processes dominate pharmacokinetic behavior during the time frame of most anesthetics. Optimal dosing in these situations requires use of all the variables of a multicompartmental pharmacokinetic model to account for drug distribution in blood and other tissues. It is not easy to intuit the pharmacokinetic behavior of a multicompartmental system by simple examination of the kinetic variables. This section examines the current state of infusion devices and the pharmacokinetic and pharmacodynamic principles specifically required for precise delivery of anesthetic agents. Rise to Steady-state Concentration the drug concentration versus time profile for the rise to steady state is the mirror image of its elimination profile. That is, in one elimination half-life an infusion is halfway to its eventual steady-state concentration, in another half-life it reaches half of what remains between halfway and steady state. The equation describing this behavior is: 702 where Cp(t) = the concentration at time t, k is the rate constant related to the elimination half-life, and t is the time from the start of the infusion. This relationship can also be described by: in which Cp(n) is the concentration at n half-lives. However, for a drug such as propofol, which partitions extensively to pharmacologically inert body tissues. With such a model, the picture changes drastically for the plasma drug concentration rise toward steady state. The rate of rise toward steady state is determined by the distribution rate constants to the degree that their respective exponential terms contribute to the total area under the concentration versus time curve. Thus, for the threecompartment model describing the pharmacokinetics of propofol, Equation 11-19 becomes: in which t = time; Cp(t) = plasma concentration at time; A = coefficient of the rapid distribution phase and = hybrid rate constant of the rapid distribution phase; B = coefficient of the slower distribution phase and = hybrid rate constant of the slower distribution; and G = coefficient of elimination phase and = hybrid rate constant of the elimination phase. For most lipophilic anesthetics and opioids, A is typically one order of magnitude greater than B, and B is in turn an order of magnitude greater than G. In contrast, with a full three-compartment propofol kinetic model, Equation 11-21 accurately predicts that 50% of steady 703 state is reached in less than 30 minutes and 75% will be reached in less than 4 hours. Manual Bolus and Infusion Dosing Schemes Based on a one compartment pharmacokinetic model, a stable steady-state plasma concentration (Cp,ss) can be maintained by administering an infusion at a rate (I) that is proportional to the elimination of drug from the body (ClE): However, if the drug was only administered by initiating and maintaining this infusion, it would take one-elimination half-time to reach 50% of the target plasma concentration and three times that long to reach 90% of the target plasma concentration. In order to decrease the time until the target plasma concentration is achieved, an initial bolus (loading dose) of drug can be administered that would produce the target plasma concentration- Although this method is very efficient in achieving and maintaining the target plasma concentration of a drug that instantaneously mixes and equilibrates throughout the tissues of the body. Obviously, the loading dose of propofol is too high, compared to clinically utilized doses (1 to 2 mg/kg) while the infusion rate appears to be a clinically acceptable dose. The erroneous estimate of the loading dose is due to the fact that the initial bolus of drug is not instantaneously mixed and equilibrated with the entire volume of tissue that will eventually take up drug. To design a manual bolus that more precisely achieves the desired target 704 plasma concentration, it is necessary to choose a bolus that is based on the small, initial volume of distribution (Vc). To maintain the target plasma concentration, a series of infusions of decreasing rate can be used that match the elimination clearance and compensate for drug loss from the central to the peripheral compartments during the initial period of extensive drug distribution and the second period of moderate drug distribution. Isoconcentration Nomogram To make the calculations of the various infusion rates required to maintain a target plasma concentration for a drug that follows multicompartment pharmacokinetics, a clinician would need access to a basic computer and the software to perform the appropriate simulations. With the appropriate formulas, this is quite feasible to do on any basic computer with any basic spreadsheet. In 1994, Shafer96 introduced an isoconcentration nomogram for propofol that used the rise toward steady state described by a multicompartmental system 705. The nomogram is constructed by calculating the plasma drug concentration versus time curve for a constant-rate infusion from a set of pharmacokinetic variables for a particular drug. By simulating a range of potential infusion rates, a series of curves of identical shape are then plotted on a single graph, with drug concentrations at any time that are directly proportional to the infusion rate. Curved lines represent the plasma propofol concentration versus time plots, resulting from the various continuous infusion rates indicated along the right and upper borders (units in g/kg/min). A horizontal line is placed at the desired target plasma propofol concentration (3 g/mL in this case) and vertical lines are placed at each intersection of a curved concentrationtime plot. The vertical lines indicate the times that the infusion rate should be set to the one represented by the next intersected curve as one moves from left to right along the horizontal line drawn at 3 g/mL. In this example, the infusion rate would be reduced 706 from 300 g/kg/min to 275 g/kg/min at 2. By placing a horizontal line at the desired plasma drug concentration (yaxis), the times (x-axis) at which the horizontal intersects the line for a particular infusion rate will represent the times at which the infusion rate should be set to the rate on the intercepting line. If it is desired that the estimated concentration never falls below the target, then the time to decrease to the next lower infusion should be at the midpoint of the subsequent interval. Extending the infusions to the subsequent midpoint times will introduce a maximum overestimation bias of approximately 17% with the illustrated infusion increments.
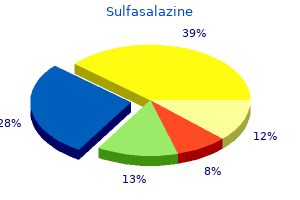
Creams milwaukee pain treatment center milwaukee wi 500 mg sulfasalazine order, ointments and oils can be used to act as emollients to reduce the drying and itching effects of the disease midwest pain treatment center fremont ohio buy 500 mg sulfasalazine visa. The skin and associated disorders Chapter 18 · · · · · · · · If infection occurs mtus chronic pain treatment guidelines 500 mg sulfasalazine purchase free shipping, then antibiotics or antifungal medication may need to be prescribed pain treatment journal sulfasalazine 500 mg order amex. In some instances pain solutions treatment center georgia discount sulfasalazine 500 mg on-line, topical steroid preparations can be used to reduce inflammation, but these should be used with caution and should not be used for longer than is necessary. Topical preparations containing both antibiotics and steroids are available, but again these should only be used for the short-term. Examples of other issues that will need to be considered are: Encourage rest as sleeping may be difficult for some patients. Dietary advice may be needed if the allergen is a food product; a multidisciplinary approach is advocated with referral to a dietician. Martin has had eczema for over 10 years; this comes and goes but is particularly bad during periods of stress. The eczema is usually symmetrical and his skin itches uncontrollably and this can have an impact on his ability to sleep. Mr Halpin has used steroid cream prescribed by his doctor; this has helped with the itching but it was less effective when the situation became severe and the itching became worse. Mr Halpin is also an asthmatic and he uses an inhaler when his breathing troubles him and this is often as a result of dust and during the winter. Currently he is experiencing itching at his elbow and in the elbow crease, and behind the knees. Red thick areas with erythema located at the back of knees and elbows are present on examination. Clinical investigations Patch testing Patch testing can be useful in helping to determine if a person is allergic to a specific substance. Small amounts of different substances are placed on the skin under an adhesive coating. The specialist nurse or doctor will then check for a skin reaction under the patches. Patch testing may help to identify the exact cause of an allergy, but it can only test for allergic contact dermatitis. It cannot diagnose other types of allergy, for example, food allergy or urticaria. On day one of testing, tiny amounts of up to 25 or more substances are applied as small patches to the skin, usually on the upper aspect of the back, fixed on with non-allergic tape. The skin is examined to determine if there is a reaction to any of the substances used. After another two days a further examination of the skin is undertaken in case the patient has a delayed reaction to any substance. If the patient has had a reaction to any of the substances, the specialist nurse or doctor will be able to tell them what it is and what materials contain that substance and the patient is given advice on how to avoid that substance. The patient should be advised to keep the area of skin being tested dry until the final skin examination, usually four days after the patches are put on the skin. The person should avoid activities that cause them to sweat a lot whilst patch testing is in progress. This skin condition has the potential to cause the patient to feel ashamed and dirty. Pathophysiologically, the cells of the basal layers of the epidermis reproduce and the more rapid upward progression of these cells through the epidermis results in an incomplete maturation of the upper layer (Weller et al. Sometimes psoriasis is associated with arthritis and this is called psoriatic arthropathy. The rash associated with psoriasis can occur when the patient is experiencing an episode of arthritis. There is often a familial history associated with this condition; Page (2006) points out that there are other precipitating/aggravating factors: · · · · · · infection (streptococcal throat infection) some medications. Skin biopsy, skin swab, throat swab and blood tests as well as clinical examination will be required the skin and associated disorders Chapter 18 to confirm diagnosis (Page, 2006). The healthcare professional has a role to play in motivating and encouraging the patient to apply the therapies meticulously, adhering to the treatment regimen. It must be noted that whatever treatment is chosen, this is not a cure for the disease and no single treatment will suit everyone and individual assessment is required: · · · · · · · · Emollients with the aim of lubricating the skin and easing scaling, as well as providing patient comfort. Coal tar ointments these preparations have an antipruritic and anti-inflammatory effect (they may stain clothing). Vitamin D analogues such as calcipotriol, tacalcitol and calcitriol; these are used amongst other things to inhibit cell proliferation. Methotrexate this is often used in the treatment of cancer; it causes inhibition of cell division. Patients should be advised to use a mat and/or grab rails in order to reduce the risk of slipping. Anybody else who may use the bath after additive emollients have been used should be warned that it will be very slippery. Case study Mark Gonzales Mark, is 20-year-old university student, arrived at the A&E department with severe second- and third- degree burns from a fire in the university halls of residence. By the time the fire brigade had arrived, and rescued him, he had suffered severe burns and was unconscious. He was transport to the A&E department with oxygen mask applied and an intravenous infusion in situ. In the resuscitation room his burns were evaluated and he was found to have primarily second-degree burns over the upper half of his posterior chest and his whole right arm including his hand. His vital signs were recorded and he was now responding, complaining of severe pain and asking what happened. Chapter 18 Fundamentals of applied pathophysiology Vital signs Physical and bloods the following vital signs were noted and recorded: Vital sign Temperature: Pulse: Respiration: Blood pressure: Observation 38. This chapter has provided an overview of the skin and has discussed a number of pathological changes that can result in disease or illness. Some of the more common skin conditions have been discussed with an emphasis on skin cancer. The reader is advised to consult other texts to fully appreciate the scope and potential the healthcare professional has in helping people with skin conditions; this chapter has merely touched on the topic. The healthcare professional has a vital role to play in assisting the individual with problems associated with the skin; however, this can only be achieved with insight and understanding. As well as the physiological disturbances resulting in problems of skin, there are also important psychological ramifications that must be given much consideration. The healthcare professional has a role to play in empowering and motivating the patient in order to adhere to prescribed treatment regimens that can often be messy and potentially damage clothing and bedding. Many patients with skin conditions and their families voice concerns about social isolation and ostracism; education and explanation may help to reduce these feelings; the healthcare professional is ideally placed to do this, acting as a key resource. This site provides easy to understand information concerning psoriasis, as well as offering information concerning research related to the condition. The charity has support groups and online forums where people can talk to others who are experiencing hair loss. They will provide impartial information, advice and support to help people feel less isolated and raise awareness to the general public and healthcare professionals about alopecia and its psychological impact. The charity supports medical and psychological researchers who aim to find effective treatments Changing Faces. Changing Faces helps people to face the challenges of living with a disfigurement and equips them with the appropriate tools to build self-confidence and self-esteem. Its work involves providing support for children, young people, adults and their families, working with schools and employers to ensure a culture of inclusion and with health and social care professionals to provide better psychological care for people with disfigurement, and campaigning for better policies and practices that are inclusive of people with disfigurements and for social change by working with the media, government and opinion leaders. Chemotherapy the use of chemical substances to treat diseases, primarily to treat cancer. The skin and associated disorders Chapter 18 Dermatoscope a magnifier with a light allowing illumination of the lesion. Relapsing (relapse) when the person is again affected by a condition that has occurred in the past. The association of use of sunbeds with cutaneous malignant melanoma and other skin cancers: A systematic review. Improving Outcomes for People with Skin Tumours including Melanoma (update): the Management of Low-risk Basal Cell Carcinomas in the Community. Learning outcomes On completion of this section the reader will be able to: · · · · Describe the functions of each of the three sections of the ear. Introduction Disorders of the structures of the head and neck range from the relatively minor to some of the most challenging you may be asked to care for. The special senses of the ear, nose and eye are something that are often taken for granted, but conditions that affect these senses can have an immense effect on the daily activities of a person. Each of these three sections is integral to the process of hearing and the inner ear is also essential to the maintenance of the sense of balance. The purpose of the oils and the wax is to lubricate the ear canal, kill bacteria and, in conjunction with the hairs, keep the canal free of debris (Lewis et al. Tympanic membrane composed of epithelial cells, connective tissue and mucous membrane. It acts as a partition between the external and middle ears and is responsible for the transmission of sound from the external to the middle ear. Middle ear the middle ear is an air space lined with a mucous membrane; it is connected to the nasopharynx by the eustachian tube, thus allowing for the equalisation of air pressure between the middle ear and the throat (and therefore atmospheric air). This equalisation of pressure ensures free movement of the tympanic membrane in response to sound waves conducted along the external ear canal. Vibrations of the tympanic membrane are conducted along the bones to the oval window; these vibrations are Chapter 19 Fundamentals of applied pathophysiology then transmitted via the oval window into the fluid of the inner ear. Inner ear the inner ear is also known as the labyrinth due to the complicated series of canals it contains (Tortora and Derrickson, 2011a). Bony labyrinth a series of cavities within the temporal bone that contains the main organs of balance (the semicircular canals and the vestibule) and the main organ of hearing (the cochlea). Membranous labyrinth a series of sacs and tubes that is contained within the bony labyrinth. Movement of the fluid within the membranous labyrinth contained within the cochlea stimulates the hearing receptors, leading to the generation of nerve impulses that are transmitted to the hearing centres of the brain (Guyton and Hall, 2010). Nose the nose is the first part of the respiratory tract and also contains the receptors for the sense of smell. The nose can be divided into external and internal sections: 566 · · External nose a framework of bone and cartilage covered by muscle and skin and lined with a mucous membrane. The external nose is divided into two airways (nares or nostrils) of roughly equal size by the septum, which forms part of the framework of bone and cartilage. Internal nose a large chamber lined with ciliated mucous membrane and containing coarse hairs that filter out large particles from inhaled air. Finer particles that enter the nose become trapped in the sticky mucus created by the membrane and are then transported to the nasopharynx by the ciliary system. The ear, nose and throat, and eyes, and associated disorders Chapter 19 air must pass over (Guyton and Hall, 2010). The internal nose has an extremely rich vascular supply, which in conjunction with the turbinates maximises the humidification and warming of the air passing through. The internal nose also contains openings (ostia) from the sinus cavities (contained within the bones of the skull). Oropharynx Tonsils the tonsils are five collections of lymphatic nodules mostly located in a ring around the junction of the oral cavity and the oropharynx (Tortora and Derrickson, 2011b): · · · two palatine tonsils located at the back of the oral cavity two lingual tonsils located at the base of the tongue a single pharyngeal tonsil (adenoid) located at the junction of the nasal cavity and the nasopharynx. The role of the tonsils is to participate in the fight against inhaled or ingested foreign substances. Hypopharynx Larynx the larynx is a short tube that connects the lower hypopharynx with the trachea. Chapter 19 Fundamentals of applied pathophysiology the mucous membrane of the larynx is formed to create two pairs of folds: 1. Ventricular folds (false vocal cords) when they are brought together, they enable the holding of the breath against the pressure in the thoracic cavity, such as when lifting a heavy object (Tortora and Derrickson, 2011b). Vocal cords (folds; true vocal cords) situated below the ventricular folds, the vocal cords are fundamental to the generation of speech. Sound is generated by the vibration of these cords, but the mouth, nasal cavity and nasal sinuses are also required to create recognisable speech (Guyton and Hall, 2010). Fibrous tunic the fibrous tunic is composed of the cornea and the sclera, and contains no blood vessels. The anterior sclera (but not the cornea) is covered by the conjunctiva, which produces a lubricating mucus that prevents the eye from drying out (Marieb and Hoehn, 2010). The ear, nose and throat, and eyes, and associated disorders Chapter 19 Vascular tunic the vascular tunic (uvea) is composed of the iris, the ciliary body and the choroid: · · · Choroid a highly vascular membrane; its blood vessels supply nutrition to all the tunics of the eye (Marieb and Hoehn, 2010). Ciliary body at the front of the eye, the choroid becomes the ciliary body a thickened ring of smooth muscle that circles the lens and has an important role in controlling the shape of the lens. Iris coloured part of the eye lying between the cornea and the lens; it contains a hole (the pupil) through which light can enter the eye. The size of the pupil is controlled by the contraction and relaxation of two separate layers of muscle fibres contained within the iris. Sensory tunic the retina has two layers; however, only the neural layer is directly involved with vision (Marieb and Hoehn, 2010). Within this neural layer are the photoreceptors: · · rods for peripheral and dim light vision cones for bright light and colour vision. Impulses generated as a result of stimulation of these photoreceptors are transmitted to the visual cortex via the optic nerve. Internal structure Internally, the eye is divided into two chambers by a barrier formed by the lens and the zonule: 1. This chamber is filled with aqueous humour, which is constantly formed and drained. The thick vitreous humour supports the back of the lens, holds the retina against the choroid and contributes to intraocular pressure, thus helping to maintain the shape of the eye (Jenkins et al. The thickness of the lens is varied by the contraction and relaxation of the ciliary muscles, depending on whether the eye is focusing on near or far objects.
Discount sulfasalazine 500 mg on-line. Arthritis rheumatoid arthritis osteoarthritis and joint pain relief with Arthro-C.
References
- Jordan GH Penile revascularization [abstract]. Presented at: American Association of Genitourinary Reconstructive Surgeons; 2005; Laguna Nigel, CA. Jordan GH: Reconstruction of the fossa navicularis, J Urol 138:102n104, 1987.
- Scott PA, Meurer WJ, Frederiksen SM, et al. A multilevel intervention to increase community hospital use of alteplase for acute stroke (INSTINCT): a cluster-randomised controlled trial. Lancet Neurol 2013;12(2):139-48.
- Cohen A, Tzourio C, Chauvel C, et al. Mitral valve strands and the risk of ischemic stroke in elderly patients. The French Study of Aortic Plaques in Stroke (FAPS) investigators. Stroke 1997;28: 1574-8.
- Hoshida Y, Li T, Dong Z, et al. Lymphoproliferative disorders in renal transplant patients in Japan. Int J Cancer. 2001;91:869-875.