
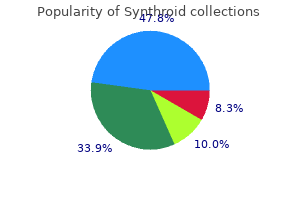
Synthroid
| Contato
Página Inicial
Ying Cheong
- Senior Lecturer, Subspecialist in Reproductive Medicine
- and Surgery, Southampton Fertility Unit, University of
- Southampton School of Medicine, Southampton
A score of 14 and above indicates a patient is a good risk for opioid therapy and those with lower scores are not considered good risks for opioid therapy medicine journey cheap synthroid 125 mcg mastercard. How often have you had to go to someone other than your prescribing physician to get sufficient pain relief from your medications How often have you taken your medications differently from how they are prescribed How much of your time was spent thinking about opioid medications (having enough medicine vicodin buy synthroid 75 mcg line, taking them treatment juvenile rheumatoid arthritis synthroid 125 mcg buy online, dosing schedule medicine man lyrics 125 mcg synthroid amex, etc medicine and manicures synthroid 50 mcg order free shipping. How often have you had to make an emergency phone call or show up at the clinic without an appointment Notes: A 17-item self-report measure to identify aberrant drug-related behaviors for patients on chronic opioid therapy. The expectations and obligations for the patient and the clinician are clearly identified and reviewed. Criteria for continued use of these medications and identification of aberrant behaviors are reviewed. The treatment decision is based on a thorough assessment with documentation of treatment rationale and the current status of the agreement. If the patient is discharged from the practice, a discussion with the patient as to the circumstances that led to this decision must take place. Directions for opioid weaning, management of withdrawal side effects, and referral to an alternate provider, be that an addictions specialist or pain specialist, should be included in this discussion with accompanying documentation. If a patient has demonstrated some aberrant behaviors or deviated from the opioid agreement, more frequent urine screens than the usual 3-month screen may be indicated. Testing procedures can be variable, and a two-step urine screen is suggested: the first step is a general screen to classify compounds using enzyme immunoassay. A positive urine drug test result is defined as the prescribed drug not present; presence of an unprescribed opioid, or the presence of an illicit substance. Cross-reactivity and false positive and negatives can confound the results of the urine screen and skew results. If the patient deviates from the opioid agreement, the clinician must decide on an appropriate course of action. There are several options that are currently being used: Discharging the patient from the practice Continuing to treat the patient without opioid analgesics Continuing to treat the patient with greater vigilance Referring the patient to a pain specialist or addictionologist Prescribing Opioid Medication Safely Elements of the opioid agreement vary in content, but generally they include the following: 1. Expected patient behaviors Prescribing Opioid Medication Safely Codeine and heroin metabolize to morphine, so both substances may be identified in urine following codeine or heroin use, resulting in a false positive for morphine. Marijuana can be detected in urine after cessation of use for up to 80 days in heavy users. Cocaine may be present in urine for 23 days if used as a topical anesthetic in dental or other procedures, and medical records should confirm this. Heroin is difficult detect due to a half-life of 530 minutes, resulting in false negatives. A small percentage of patients metabolize opioid, especially oxycodone, rapidly resulting in a false negative for this drug. The elements of this two-page follow-up assessment tool include the following: Current analgesic regime Level of analgesia; average, worst, amount of pain relief from medications Activities of daily living; physical, family and social relationships, mood, and sleep Adverse events Understanding Aberrant Behaviors Some patients who are taking opioids regularly to manage chronic pain can develop aberrant behaviors that may or may not indicate addiction. These behaviors may have a different source such as unrelieved pain related to undertreatment, or financial concerns. Behaviors that are more predictive of addiction include concurrent use of illicit drugs, stealing or selling prescription drugs, injecting oral medications, repeated resistance to changes in therapy although there are clear negative effects, and deterioration in family and work relationships related to drug use. Validation of a screener and opioid assessment measure for patients with chronic pain. The impact of pain on quality of life and the unmet needs of pain management: results from pain sufferers and physicians participating in an Internet survey. What percentage of chronic nonmalignant pain patients exposed chronic opioid analgesic therapy develop abuse/addiction and or aberrant drug-related behaviors Substance abuse disorders in a primary care sample receiving daily opioid therapy. Universal precautions in pain medicine: a rational approach to treating chronic pain. Addiction-related assessment tools and pain management instruments for a screening, treatment planning, and monitoring compliance. A new tool to assess and document pain outcomes in chronic pain patients receiving opioid therapy. Pain Management: Noninterventional Rehabilitation-Based Spectrum of Care Steven Stanos the primary care clinician serves a valuable role in assessing, managing, and facilitating a wide range of pain-related conditions. This role includes the assessment of acute injuries, for which appropriate assessment and treatment can be critical to patient quality of life. A more disease-centered approach may be more applicable to chronic conditions where consideration of biological, psychological, and social issues may also be entertained. This chapter will review issues related to assessment and goals for acute, subacute, and chronic pain. Finally, tips regarding when and how to more effectively utilize referrals to other specialists will be discussed, including the role of pain management specialists, physiatrists, and addiction medicine. Therapy Professionals Proper referral to therapy professionals is an important function of the primary care provider, and like other clinical referrals made, can help to determine the success of an intervention and improved outcomes for the patient. Allied health professionals commonly used include physical and occupational therapist, pain psychologists, counselors, relaxation specialists, and nurse educators (Table 13. Physical and occupational therapists are the principal members of the rehabilitation team that helps restore structure and function to injured patients suffering from painful conditions. Occupational therapy focuses on educating patients regarding proper posture and ergonomics related to functional activities. In some settings, occupational therapy may focus more on upper extremity disorders, activity of daily living, and work rehabilitation issues. Many times, therapists from different areas may work together or "co-treat" as a means of improving patient-specific outcomes with therapeutic collaboration. Physical and occupational therapists employ the use of passive and active therapeutic exercises and passive modalities in guiding patients through the process of tissue recovery and rehabilitation. Targeted therapeutic exercises are utilized to address specific deficits in posture, flexibility, strength, balance, neuromuscular coordination, and endurance. Passive modalities such as cryotherapy, heat, and electrical stimulation are commonly used to address pain, alter tissue distensibility, and control inflammation. Patient and family/caregiver education may be an additional component of the long-term pain management program. Referring a patient with acute or chronic pain to physical therapy is common practice for all practitioners. A number of factors should be considered in order to better improve the chances of a successful outcome for the patient. Key considerations may include accessibility, timeliness for evaluation, level of skill and specialty training in the facility, appropriate delivery of services, and communication between referring clinician and the facility. A referral to physical therapy usually includes an order or prescription for services. The initial visit usually consists of a comprehensive evaluation, which includes a condition-specific history and physical exam by the therapist. Prognosis and short-term and long-term goals are included in the evaluation report, which is usually forwarded back to the ordering clinician where the order can be signed off and /or modifications or suggestions can be made. In some states, a physical therapist may be licensed to practice without referral from a physician or medical practice. Therapy units are usually set on 15-minute intervals (units) where patients are seen individually for 1 hour (4 units). Progress, response to treatment, and monitoring of compliance are important parts of subsequent therapy notes that should be communicated back to the referring physician. Facilities that rely heavily on excessive use of passive modalities (ice and heat packs, ultrasound, and massage) may not offer the patient any long-lasting benefits from a therapy program. Be cautious of facilities that include an evaluation by a physical therapist, but subsequent visits are done by a therapy extended provider. The therapist should provide written instructions, exercise logs, and appropriate multimedia support to help advance the patients. Pain psychology assessment and intervention focuses on both cognitive and behavioral factors related to pain. Psychological intervention is focused on unlearning maladaptive responses and reactions to pain while fostering wellness, improving coping, perceived control, and decreased catastrophizing. Pain psychology interventions also focus on pain-related anxiety, depression, and anger. Behavioral and cognitive-behavioral interventions include a wide spectrum of treatments focusing on changing behaviors, thoughts, and feelings related to chronic pain. These include traditional cognitive restructuring, behaviorally based activity planning and management, problem solving and skills training, relaxation training. The primary care provider may be an important facilitator or point person for managing the patientspecific case or may use more structured multi- or interdisciplinary models depending on patient needs. Asking the patient to describe and demonstrate exercises or stretches learned in therapy can be an important part of subsequent follow-up visits with the clinician. Cognitive therapy: also know as cognitive restructuring or self-statement analysis, including behavioral experiments 4. Behavioral activation and management, including goal-setting and pacing strategies 5. Other interventions to change perception or emotional responses to pain, such as guided imagery, desensitization, hypnosis, or attention control exercises 7. Behavioral and cognitive behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. These models include, in order of increasing comprehensiveness and philosophical complexities: parallel, collaborative, coordinated, multidisciplinary, interdisciplinary, and finally, integrative approaches. An example includes the various allied health and health care providers working in an emergency. Moving across the continuum, more collaborative models include a case manager helping to facilitate treatment between the patient and physician. More collaborative models involve less hierarchy and more communication between health care practitioners. Acute pain and musculoskeletal injuries may also be managed by a more simple collaborative approach. In multidisciplinary treatment, the primary care provider may serve as the referral organizer, managing medication issues for a patient and referring to other professionals, such as physical therapy, for additional treatment. In multidisciplinary models, treatment is delivered at different facilities with minimal formal communication. This model is the most commonly used in the primary care setting, and relied on the primary care provider to manage most medication issues and make decisions regarding continuation of other therapies as well as possible referral to interventional specialists and surgeons. A more collaborative interdisciplinary model involves a number of specialists working in one facility, who are able to communicate and collaborate on an ongoing basis to better improve patient outcomes. This type of formal pain program is usually led by a pain physician or psychologist and delivered in an outpatient or inpatient setting. A recent study of fibromyalgia patients found slow breathing reduced ratings of pain intensity, unpleasantness, and negative affect ratings in experimentally produced thermal pain. Biofeedback is a self-regulation technique that has been found to be effective in a number of chronic pain conditions, including headache and myofascial pain. These physiologic and measurable responses or "bio" are monitored and brought to awareness by the patient. As the patient learns the specific skill or technique, he or she continues to practice and improve the intervention individually. Relaxation therapy uses similar "feedback" techniques to induce a relaxation response and include deep or diaphragmatic breathing, progressive muscle relaxation, guided imagery, and certain types of meditation and yoga. As training progresses, patients develop an enhanced awareness of the body and a greater ability to relax more easily and in a shorter time frame. Techniques include self-control meditation (a shortened form of progressive muscle relaxation), paced respiration (the patient breathes slowly and deliberately for a specific time period), and deep breathing (the patient takes a deep breath, holds it for 3 to 5 seconds, then slowly releases it). Relaxation therapies are easy to learn, utilize minimal health care resources, and are without side effects. However, they can be very powerful tools for the patient with persistent pain and elevated levels of anxiety and related muscle tension Meditation Some practitioners consider meditation to be a deep method of relaxation therapy. Although various forms of meditation are practiced, common forms include mindfulness meditation, transcendental meditation, yoga, and walking meditation. Mindfulness mediation is more commonly being used in pain medicine and involves the patient concentrating on body sensations, thoughts, or emotions that occur "in the moment. Over time, meditation should be associated with less anticipation and negative view of pain. Yoga and walking meditation, derived from Zen Buddhism, focuses on controlled breathing with slow deliberate movements and postures. Transcendental meditation is similar but also focuses on a repetitive sound or thought, with the repetition of a word or sound. Common visualization of a safe place includes imagery of a peaceful location or more physiologically focused imagery such as imagery of fighting disease. A recent study found guided imagery with relaxation as a useful technique in a study of osteoarthritis patients, demonstrating reduced pain, improvement in mobility, and reduction in the use of over-the-counter medications. Early referral can include referral to a specialist for interventional therapies, acute surgical emergencies. Many times, after initial conservative measures have failed or offered minimal analgesic or functional improvements, referral to a pain specialist may be necessary. A number of additional reasons besides inadequate or suboptimal pain reduction may include comorbid psychiatric disorders limiting response to treatment, need for diagnostic evaluation, and /or validation of treatment plan. In management of acute and chronic pain with opioids, increased aberrant behaviors, problematic use of medications, or signs of addiction or medication misuse may be critical signals to refer the patient to an experienced medical management pain specialist for transfer of care or consultation. Early intervention and referral may help to limit the development or progression of chronic pain and related affective distress, as well as limited unnecessary suffering by the patient due to suboptimal care. If initial interventions by the primary care provider provide limited or no benefit, referral to a pain specialist may be the next option. A more disease-centered approach, common in other areas of primary care, that is, diabetes, hypertension, is needed for subacute and chronic pain conditions. The approach includes a more comprehensive assessment of pertinent biological, psychological, and social issues. A wide range of health care providers, including physical and occupational therapists, pain psychologists and counselors, vocational rehabilitation therapists, nurse educators, and other complimentary medical providers, may help the primary care provider develop a patient-specific treatment program facilitated by the use of theses team members. Pain psychology interventions may include behavioral and cognitive-behavioral approaches as well as mindbody-focused treatments.
When associated with cutaneous burns treatment degenerative disc disease synthroid 25 mcg without prescription, smoke inhalation doubles the risk of mortality symptoms dehydration discount synthroid 125 mcg overnight delivery. If the patient is receiving 100% O2 medicine 91360 order synthroid paypal, the half-life is reduced to approximately 40 to 60 minutes medications questions purchase discount synthroid online. Resuscitation Cutaneous burns produce accelerated fluid loss into the interstitial tissues in the burned and nonburned areas medications 7 synthroid 200 mcg order on-line. Mediators such as prostaglandins, thromboxane A2, and reactive oxygen radicals are released from injured tissue, which cause local With these large burns, an initial decrease in cardiac output is seen, followed by a hypermetabolic response. Organs, including skin, can progress from a hypoperfused state to more permanent end-organ damage if resuscitation is not accomplished in a timely fashion. For larger burns, isotonic intravenous fluids such as lactated Ringer solution should be used (large volumes of normal saline can cause hyperchloremic metabolic acidosis). Fluid needs are estimated by the Parkland or other formulas such as the Modified Brooke formula. Based on the Parkland formula, for adults and children weighing more than 10 kg, the total 24-hour volume is calculated using 4 mL/kg/% burn. Half of this amount is given in the first 8 hours and the remainder in the next 16 hours. Intravenous fluid hydration given by the paramedics en route should be considered part of this volume. Children weighing less than 10 kg should be given 2 to 3 mL/kg/% burn divided similarly over the next 24 hours. Because of the increased capillary permeability, colloids such as albumin are generally avoided for the first 12 to 18 hours but can be used subsequently if resuscitation is not being achieved with the crystalloid regimen. Inhalational injuries, extensive and/or deep burns, and delayed resuscitation usually result in larger fluid requirements than initially calculated. Patients should not be massively fluid overloaded during the resuscitative period. The body can be fairly accurately divided into anatomic regions that represent 9% or multiples of 9% of the total body surface. As burns marginate, the assessment of depth may change from the value calculated initially, particularly in the case of scald burns, where the initial depth may not appear as severe. Fourth-degree burns are those that extend through skin and subcutaneous fat, even involving deep structures. Excise and graft deep dermal burns Seconddegree or partialthickness Through epidermis and into dermis Pink/red, weepy, swelling and blisters, very painful Third-degree All the way or fullthrough thickness dermis White or dark, leathery, waxy, painless Excise and graft Prophylactic intravenous antibiotics are usually not recommended because they select for resistant organisms. The different creams commonly used topically have local broad antimicrobial activity that can resist colonization. Furthermore, it can cause severe systemic metabolic acidosis through carbonic anhydrase inhibition. It penetrates the eschar and is therefore useful for full-thickness infected burns (there is less pain on application) and for unexcised burns with colonization. Usage can result in severe leaching of sodium and chloride, which can lead to profound hyponatremia and hypochloremia, particularly when used on large areas on children. These responses include the activation of the complement and coagulation pathways producing microvascular thromboses, capillary leak, and interstitial edema. The systemic activation of the proinflammatory cascade also triggers subsequent counter-regulatory anti-inflammatory reactions that produce subsequent immune suppression and increased susceptibility to nosocomial infections and sepsis. Neurologic: Transient delirium commonly occurs, but an altered mental status requires evaluation to identify other etiologies such as anoxia and metabolic abnormalities. Pulmonary: Pneumonias and respiratory failure requiring mechanical ventilation are frequently seen. Cardiovascular: Myocardial depression occurs transiently following major burns, and this is mediated by vasoactive and inflammatory mediators released by the injured tissues. In selective patients, inotropic agents to support end-organ perfusion are indicated during the early postinjury period (initial 24-48 hours). Suppurative thrombophlebitis can lead to bacteremia, which may cause endocarditis along with the local venous abscess. Gastrointestinal: Stomach and duodenal ulcers can develop secondary to decreased mucosal defenses resulting from the decrease in splanchnic blood flow. Early gastric tube feedings before atony occurs may help improve nutrition or prevent stress ulcers. Early feeding may prevent the development of nosocomial pneumonias by inhibiting bacterial overgrowth. As the result of regional hypoperfusion, critically ill burn patients are at risk for the development of acalculous cholecystitis, pancreatitis, and hepatic dysfunction. Renal: Acute kidney injury is reported in up to 20% of patients with severe burns. Early on, acute tubular necrosis can develop because of inadequate resuscitation or myoglobinuria (commonly associated with deep burns and electrical injuries), and late onset of acute kidney injury can be caused by sepsis, worsening of preexisting renal dysfunction, and nephrotoxic agents (eg, medications and contrast media). Infection: Burn size and increased age are contributors of host immune suppression and increased susceptibility to infections following major burns. Infections can arise from the burns themselves or from treatments used in critical care, such as urinary tract infections from Foley catheters and sinusitis or otitis from feeding or nasogastric tubes. Ophthalmic: Corneal abrasions or ulcerations may be seen, resulting either from the initial injury or from exposure. Patients with potential eye injuries, particularly those caused by explosions, should be examined early in the emergency department using fluorescein for corneal abrasions, which should be treated with antibiotic lubrication. Musculoskeletal and soft tissue: Scarring can cause functional or cosmetic defects. Physical and occupational therapy, scar releases, regrafting, and silicone prostheses can help. Because of the specialized care required and the multidisciplinary aspects of burn treatment, the American Burn Association recommends that certain patients receive their care at burn centers (Table 133). In most cases, these goals can be accomplished with appropriate home care, outpatient physical therapy, and frequent outpatient follow-ups. Excision of entire burn wound with autologous split-thickness skin graft application B. Burn wound excision and split-thickness skin graft coverage to be performed in three separate stages C. Excision of burn wound with application of cadaveric skin for temporary coverage, followed by definitive coverage with autologous skin graft in 8 days D. Application of silver sulfadiazine to wound until epithelialization of wound is complete E. Excision of burn wound and application of full-thickness autologous skin graft 13. A 55-year-old man with second- and third-degree burn to the anterior chest and abdomen sustained when his clothes caught on fire at a barbecue D. A 3-year-old boy with a scalding burn to the left forearm after he accidentally pulled a pan of hot grease of the stove and whose mother is extremely tearful and guilt-ridden E. A 30-year-old man with second-degree burns to the anterior abdomen and both thighs anteriorly 13. Lactated Ringer solution at 350 mL/h for the initial 8 hours followed by an infusion rate of 700 mL/h for the next 16 hours C. Lactated Ringer solution at an initial rate of 700 mL/h for the first 8 hours followed by an infusion rate of 350 mL/h for the next 16 hours D. Lactated Ringer solution at 700 mL/h over the first 8 hours and infusion to titrate to an hourly urine output of greater than 0. Early excision of the burn wound followed by autologous partial-thickness skin graft application is the most appropriate definitive wound management approach for this patient, because this approach reduces septic complications associated with wound sepsis, and early skin grafting also provides patients with the best functional recovery. Staged burn wound excision and skin graft coverage is another strategy applied for patients who do not have sufficient autologous skin for initial coverage. Definitive treatment of burn wounds with dressing changes and healing by secondary intention (wound contraction) is not acceptable for most burn patients because of increased wound infection risks associated with uncovered burn wounds and because of the poor cosmetic and functional results associated with this type of healing. Full-thickness skin graft has the advantage of having greater tensile strength and works best for coverage of areas that are susceptible to trauma, such as the foot or weightbearing surfaces. However, the disadvantage of full-thickness graft is problems with donor sites that may require additional coverage. The Parkland formula recommends an initial fluid resuscitation over the first 24 hours after a major burn to consist of lactated Ringers solution with a 24-hour volume = 4 mL/kg/% burn. Half of this calculated volume is recommended for the first 8 hours, followed by infusion of the remaining 50% of the volume over the next 16 hours. A patient who does not respond to initial fluid resuscitation with the calculated fluid amount should be reassessed for possible complicating factors, including coronary artery disease, intrinsic renal disease, and possible miscalculation of burn wound size. The infusion of colloids such as albumin may potentiate capillary leak and tissue swelling during the initial 8 hours of resuscitation. Dopamine therapy should not be initiated until intravascular volume has been adequately restored. Sulfamylon application may cause metabolic acidosis, as demonstrated by the arterial blood gas. Another unattractive quality associated with Sulfamylon is that it causes pain when applied. The patient says his symptoms have been present for the past 12 months and have progressively worsened. The patient currently has pain and tightness in both calves that develop after walking less than one block but routinely resolve after a short period of rest. The popliteal, dorsalis pedis, and posterior tibial pulses are absent bilaterally. Know the differential diagnosis for claudication caused by arterial insufficiency. Be able to recognize the indications for lower extremity revascularization and the benefits and limitations of open surgical and endovascular techniques. Learn the noninvasive modalities available for the evaluation and follow-up of patients with claudication. Patients with claudication are at risk for the developing complications related to the lower extremities, as well as coronary and cerebral vascular complications. Aspirin has not been shown to improve claudication but has been shown to reduce the risk of myocardial infarctions, strokes, and the progression of claudication symptoms. The antiplatelet agent, clopidogrel is more effective than aspirin in the prevention of cardiovascular ischemic events; however, this medication is associated with increased cost and increased bleeding complications. Lipidlowering medications (statins) have been found highly effective in reducing the risk of major cardiovascular events in patients with peripheral vascular disease. For patients with more advanced stages of ischemia, interventional treatment for limb salvage becomes the desired goal. More advanced disease generally implies more anatomic levels with occlusive or stenotic pathology. Acute ischemia is typically characterized by a sudden onset of pain, pallor, and pulselessness. Chronic arterial ischemia manifests as lower extremity pain with exercise and resolves with rest. In general, the outcomes after intervention are better with type A lesions with worsening outcomes from A to D. Neurogenic claudication can occur in association with lumbar stenosis, which can also produce excruciating lower extremity pain during exertion or positional changes; however, the onset of neurogenic claudication symptoms tends to occur more sporadically and may require positional changes for symptom improvement. Physical examination findings such as skin temperature, capillary refill, and peripheral pulses are useful to help differentiate patients with neurogenic symptoms from those with ischemic symptoms. Increasing levels of arterial involvement usually suggest a greater need for interventional therapy. Additionally, the susceptibility of a diabetic patient to infection can enhance the risk of tissue loss. The use of clopidogrel is, however, associated with higher cost and slightly increased rate of treatment-related complications. Because any surgical or endovascular intervention can cause possible limb- or life-threatening complications, the clinician needs to weigh the risks and benefits of intervention for a patient with claudication differently than for a patient with digital gangrene. The patient with claudication should be severely disabled and not merely inconvenienced before being considered for either endovascular treatment Conversely, the patient with digital gangrene is in a limbthreatening situation, requiring definitive revascularization if the limb is to be salvaged. A patient with claudication with severe lifestyle limitations (such as the loss of a job) may be a candidate for revascularization if the risk profile is not too unfavorable. Angioplasty techniques work best for proximal vessels with short, focal, concentric, noncalcified atherosclerotic stenosis. In selective cases, when there is residual gradient or dissection following angioplasty, stent placement may help improve short-term patency. The more unfavorable the lesion is with respect to length, number, location, and morphology, the less successful percutaneous therapy will be. Percutaneous treatment of occlusive disease at the femoropopliteal level is being increasingly utilized as technological advances are being introduced. As a general rule, outright arterial occlusions require bypass to achieve revascularization. More proximal-level bypasses at the aortoiliac level can achieve 90% 5-year patency, whereas distal femoral-tibial bypasses can achieve less than 65% 5-year patency. He is a diabetic and takes an oral hypoglycemic agent, a longacting -blocker, and a statin-class lipid-lowering agent. He returns after 8 months with continued calf pain, as well as nonhealing ulcers between his left third and fourth toes. Her physical examination reveals normal temperature, normal femoral pulses, diminished left popliteal pulse, and nonpalpable left pedal pulses. Her right lower extremity vascular examination reveals normal femoral pulse and diminished popliteal and pedal pulses. Her left great toe and second toe have dark eschars at the tip with surrounding erythema extending to the mid-foot. Obtain an angiogram of the aorta and left lower extremity to identify the areas of occlusion and treat the blockage with angioplasty and stent placement.
When medications are combined symptoms anemia purchase synthroid with amex, especially in patients already on other treatments for chronic diseases medicine hunter order discount synthroid online, the risk of side effects medicine hat horse synthroid 200 mcg purchase overnight delivery, drugdrug medications hypertension buy synthroid 100 mcg, and diseasedrug interactions become much more likely treatment centers in mn generic synthroid 125 mcg on-line. Tapentadol also does not utilize the cytochrome P450 systems, which means far fewer drugdrug interactions. One of the benefits of tapentadol appears to be fewer side effects, especially nausea and vomiting, compared to traditional opioid therapy. Tapentadol has not been studied in low back and neck pain, but opioids have shown moderate effects in these conditions. A survey of primary care physician practice patterns and adherence to acute low back problem guidelines. Managing low back pain-a comparison of the beliefs and behaviors of family physicians and chiropractors. New insights into the mechanism of action of acetaminophen: its clinical pharmacologic characteristics reflect its inhibition of the two prostaglandin H2 synthases. Overexertional lumbar and thoracic back pain among recruits: a prospective study of risk factors and treatment regimens. Nonsteroidal anti-inflammatory drugs for low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. A comparison of the efficacy and safety of nonsteroidal antiinflammatory agents versus acetaminophen in the treatment of osteoarthritis: a meta-analysis. Over-the-Counter Drug Products Containing Analgesic/Antipyretic Active Ingredients for Internal Use. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Does gabapentin have an analgesic effect on background, movement and referred pain Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration. Therapy of acute lumbovertebral syndromes through optimal muscle relaxation using diazepam. Opioids for chronic noncancer pain: a meta-analysis of effectiveness and side effects. A comparison of the efficacy and adverse effects of controlled release dihydrocodeine and immediate release dihydrocodeine in the treatment of pain in osteoarthritis and chronic back pain. Efficacy of 12 hourly controlled-release codeine compared with as required dosing of acetaminophen plus codeine in patients with chronic low back pain. Comparison of the efficacy and tolerability of a paracetamol/codeine fixeddose combination with tramadol in patients with refractory chronic back pain. Short-term efficacy of intravenous pulse glucocorticoids in acute discogenic sciatica. Prolapsed lumbar disc treated with intramuscularly administered dexamethasonephosphate. When deciding which type of pain referral to make, the health care practitioner should carefully consider the type of pain that the patient has. If a patient with low back or neck pain has a radicular component to his or her pain, a good option for referral would be an anesthesia-based pain clinic where epidural steroid injections are performed regularly. Approximately 50% of patients referred to a pain clinic with neck pain have facet-related pain, which can respond very well to a facet injection. However, currently data indicate that there are only 6 board-certified pain specialists for every 100,000 patients. Most health care practitioners tend to attempt to manage pain in their patients with a combination of medications, physical therapy, or other treatment options such as heat or cold packs. For many patients this approach will work, but only 58% of patients with chronic pain are satisfied with their analgesics. An interventional option may be needed to help relieve or decrease pain and increase functionality in patients who have failed medication therapy and still report high levels of pain. In general, a pain clinic referral is indicated when the following occur: Multiple medications and doses have been tried, without good result. No matter what type of pain or intervention is being considered, the patient who is referred to the pain clinic will have a multidimensional pain assessment and evaluation process that will help determine just what type of treatment will benefit the patient Common Interventional Pain Management Options Most interventional pain clinics have the ability to perform a group of common interventional pain treatment techniques. As a part of the comprehensive pain assessment and evaluation process, the patient will need to provide information on the following: Medical history Surgical history Past pain experiences Any history of a substance abuse disorder, alcohol use, or previous illicit drug use Psychiatric history Medication use history Laboratory findings Imaging results. An important contraindication for injection therapy is infection or anticoagulation. It is caused by a loss of height or shrinking of the disk or vertebra, causing laxity in the facet joint. As with other types of injection, there is a diagnostic phase where two injections can be performed at 2-week intervals and then in the treatment phase the interval should be 4 to 6 weeks. In the case of cervicogenic headache, procedures may take place at intervals of 6 weeks after the treatment phase is completed. The use of a cervical facet block with a local anesthetic and steroid in the intra-articular facet space can be beneficial. In a randomized controlled study with bupivacine alone or bupivacaine and steroid pain reduction lasted for 14 to 16 weeks in both groups. Facet Injection Cross - section of facet joint showing injection into the joint cavity. Epidural Steroid Injections Since low back pain and neck pain are common pain complaints for patients, 70% to 80% and 60%, respectively, at some point in their lifetime, many patients will be offered and receive an epidural steroid injection. It can reduce the time to perform the block, number of attempts, and reduce block onset time. Once the site for injection is located, a needle is then inserted through the back into the epidural space of the spinal column and a solution of local anesthetic and steroid is injected. The most commonly used local anesthetics are bupivacaine and ropivacaine, and depomedrol is a commonly used steroid. The effect of the injection is not immediate in most cases and it may take 57 days for the full effect to take place. The suggested injection interval is 1 to 2 weeks in the diagnostic phase and then 2 months if greater than 50% pain relief is achieved with the first series of injections. A Cochrane review, indicates no evidence for pain relief for chronic or subacute low back pain. This does not mean that these techniques are not supported by outcomes, just that there is not enough strong research to support practice recommendations. Sacroiliac Injections When a patient has low back pain or leg pain there should be high suspicion that the sacroiliac joint is the pain generator. It has a large number of nerves that can become compressed or irritated causing low back or leg pain. Myofascial pain syndrome is one pain condition where a localized injection has shown some efficacy. To perform the procedure, local anesthetic (Lidocaine) is injected directly into the painful area. The drawback to the technique is the short-term pain relief that the injection provides. Botulinum Toxin (Botox) Injections Botulinum toxins are a product of the anaerobic bacteria Clostridium botulinum. To use a Botox injection for cervical dystonia, the toxin is injected directly into a muscle with muscle weakness occurring within 2 weeks. Patients have reported that the pain from an injection is higher than the blocking effect. In a study of plastic surgery patients who received Botox for cosmetic purposes, 51% of 77 patients with migraine reported complete relief of headache and 38% of 77 patients reported partial relief. These Prolotherapy or Regenerative Injection Therapy the injection of an irritant solution such as dextrose/phenol/glycerine or pumice into weakened back muscles has been found to provide pain relief when combined with an aggressive physical therapy regimen. Radiofrequency Lesioning, Intradiscal Electrothermal Therapy these therapies use a heated probe to transect the nerve in the painful area. This practice has provided anecdotal reports of pain relief for discogenic back pain. Attached to the scope are tools that can be used to remove scar tissue from nerve roots that has been found to be a source of inflammatory pain. There is insufficient research to indicate whether the riskbenefit ration of this technique merits its use. Implanted Modalities Intrathecal drug delivery systems are used to control intractable chronic pain or malignant pain in patients. Since the techniques are considered to be secondary or third-tier options, there is limited research available and support may not be strong for these techniques as a result. This does not mean the techniques have no value, just that the literature to provide research support has not yet been developed. In order to permanently place an implanted pump, a trial of the technique is performed to determine efficacy of the modality. An implanted computerized pump automatically delivers a prescribed dose of medication at a set rate. Morphine is the most common medication and using an intrathecal medication delivery can provide morphine doses that are 300 times as potent as oral morphine. These include the following: Depression Cognitive impairment Depressed levels of consciousness Hallucinations Elevated creatinine kinase levels. Patients who receive Prialt should be evaluated prior to use for any current psychiatric conditions that would preclude the use of the drug. They should also be carefully reassessed after the treatment begins for any signs of adverse events. The use of an intrathecal medication delivery system can have any number of problems. The patient riskbenefit ratio should be carefully weighed and all other reasonable options should be tried before the pump implantation is tried. If during the trial the patient does not have a 50% reduction in pain levels, pump placement should be reevaluated. There is strong evidence for use of implanted pumps for short-term improvement of malignant or neuropathic pain. During the trial period, the drug selection is based on the following: History of opioid tolerance Side effect history Pain afferent spinal cord level compared with catheter tip location. As the pain stimulus continues to present itself to the neuron, the gate opens to transmit the pain stimulus. Spinal cord stimulation acts to selectively depolarize large fiber afferents in the dorsal columns of the spinal cord closing the gate without causing motor effect. When the system is activated, the patient will feel a tingling, or paresthesia, over the affected or painful area. For patients with neck and back pain a multimodal approach including interventional options can provide optimal pain relief. Sending the patient with these conditions to a pain specialist does not mean an injection or interventional technique will be used. In other cases the addition of an intervention can provide the added pain relief the patient needs to participate more fully in the plan of care and rehabilitation. Guidelines for the proper use of epidural steroid injections for the chronic pain patient. Medications for acute and chronic low back pain: a review of evidence for an American Pain Society/American College of Physicians Clinical Practice Guideline. Botulinum toxin intramuscular injections for enck pain: a systematic review and metaanalysis. A randomized, double blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Many of these patients will be taking opioids, either short-acting or extended release preparations. They may also be taking these medications long term over the course of several years. In addition, they may be using other co-analgesic medications such as antidepressant or neuropathic pain drugs. This means that many will be heavily opioid dependent and have complex analgesic needs while they are hospitalized for their surgery. In many cases, this may be the outcome, but in other instances the back or neck pain may not improve and may even worsen. For patients for whom surgery is successful, a better quality of life is possible. For the remainder of the patients for whom surgery is not fully successful, depression may increase or the patients may feel disappointment about having an additional procedure without the benefit they had planned. When patients with back and neck pain are considering a surgical procedure, it is important to set the right expectations. This involves a real and complete explanation of the process and a frank discussion with the patient about the potential outcomes of the procedure. By setting realistic expectations with the patient in a preoperative setting, the patient will be more relaxed and accepting when the outcome is not perfect immediately after surgery. Patients should also consider how their chronic pain and the medications they take for pain management will affect their surgical experience. For example, patients who are taking opioids for a period of more than 4 weeks prior to surgery should expect that the amount of medication needed to control their pain after surgery will be higher and pain relief may be more difficult to achieve. It is also important to remember that patients with long-term pain have had many experiences with the health care system. Some will have been successful, while others may have been very demeaning, for example, incidences when they may have been labeled as addicted or drug seeking. Building a trusting relationship requires an honest and forthright approach to questions and patient concerns. Inpatient Issues Patients with chronic pain are more difficult to treat for surgical pain in the postoperative setting only because there are complex pain management needs that need to be addressed. These complex needs can include the following: Tolerance to opioids Physical dependence on opioids for chronic pain relief the need for higher doses of pain medication to control postoperative pain1,2 the American Society of Anesthesiologists has recommendations for controlling pain in the perioperative period.
Syndromes
- Trouble breathing, wheezing, shortness of breath
- Triglycerides
- You develop symptoms of long-term liver damage
- Chemotherapy uses drugs to kill cancer cells and stop new cells from growing.
- High blood pressure
- Failure to respond to luteinizing hormone releasing factor
In rare instances symptoms chlamydia generic 100 mcg synthroid overnight delivery, especially when edema develops suddenly and severely medications side effects prescription drugs generic synthroid 100 mcg buy online, frank rupture of the skin with extravasation of fluid may result medications prescribed for depression cheap synthroid 50 mcg buy online. Edema is usually more marked on the paralyzed side of patients with hemiplegia; unilateral edema may also result from unilateral venous obstruction medications quetiapine fumarate buy synthroid online. She exhibits many of the typical demographic features including advanced age medications you cant take while breastfeeding generic synthroid 25 mcg without prescription, a history of hypertension, and elevated body mass index as well as clinical signs and symptoms of decompensated heart failure. Although aggressive management of hypertension in this disorder is beneficial,1 no specific therapy has been clearly associated with a survival benefit. After randomization to irbesartan or placebo there was no significant effect on mortality or hospitalizations from a cardiovascular cause. The excess volume of extracellular fluid is a more important determinant of edema. In adults, a minimum of 4 liters of excess extracellular fluid volume usually must accumulate before peripheral edema is manifested. In patients with chronic left ventricular failure and a low cardiac output, peripheral edema may develop in the presence of normal or minimally elevated systemic venous pressure because of a gradual but persistent accumulation of extracellular fluid volume. A report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines: Developed in collaboration with the International Society for Heart and Lung Transplantation. Characteristic findings include jugular venous distention, hepatomegaly, peripheral edema, accentuation of the P2 component of S2, gallop heart sounds (in particular, an S3) and pulmonary rales. Chronic, marked elevation of systemic venous pressures may result in severe tricuspid regurgitation with visible systolic pulsation of the neck veins and even the eyes. Low cardiac output results in sympathetic nervous system activation and systemic arterial vasoconstriction, which helps to support blood pressure and maintain endorgan perfusion. Sustained arteriolar vasoconstriction commonly produces pallor and coldness of the extremities and, in severe cases, digital cyanosis. In patients with mild right-sided heart failure, the jugular venous pressure may appear normal at rest but may rise with compression of the right upper quadrant. Formally, a positive abdominojugular reflux test is defined as a sustained increase in jugular venous pressure of >3 cm that persists during prolonged abdominal compression (up to 1 minute). If present, this sign indicates that intracardiac filling pressures are elevated and the right side of the heart is unable to accommodate increased venous return. Hepatomegaly is a common finding in patients with heart failure and often occurs before lower extremity edema develops. If hepatomegaly occurs rapidly, as in cases of sudden onset of heart failure, acute stretching of the liver capsule ensues that can result in right upper quadrant tenderness. However, in long-standing heart failure this tenderness abates, even if the liver remains enlarged. Ascites may follow as a result of increased visceral capillary permeability, long-standing systemic venous hypertension, and hepatic venous congestion. Rarely, persistent visceral congestion due to severe heart failure may result in a protein-losing enteropathy. The resultant reduction in plasma oncotic pressure may exacerbate the underlying tendency to form ascites. Repeated hospitalizations for heart failure, hyponatremia, intolerance to beta-adrenergic blockade, and a markedly reduced peak oxygen uptake of 10 mL/kg/min are all markers of poor prognosis and, taken together, predict mortality >50% in the next year. Such a patient should be considered for advanced therapies, including heart transplantation and mechanical circulatory support. Given the limitations of donor supply, cardiac transplantation is generally reserved for younger patients with few comorbid conditions. In addition, because of renal insufficiency and the recent diagnosis of cancer, this patient is unlikely to be eligible for transplantation (either heart alone or combined heart-kidney). Furthermore, the typically long waiting time for a donor heart renders transplantation an impractical immediate solution for this patient with a very limited predicted short-term survival. Mechanical support can be used as a "bridge to transplantation" and also as permanent "destination therapy" in patients for whom cardiac transplantation is not feasible. Such devices may also be used as a "bridge to recovery" in rare cases of an identifiable, potentially reversible cause of cardiac decompensation, such as acute myocarditis, postcardiotomy syndrome, or peripartum cardiomyopathy. Because this patient is ineligible for transplantation, destination therapy would be the most appropriate mechanical support strategy. Food and Drug Administration both as a bridge to transplantation and as destination therapy. Continuousflow pumps are relatively low profile devices that allow implantation in smaller patients and offer mechanical durability but do expose patients to the risk of stroke, infection, and bleeding. Although mechanical biventricular support is also available as a bridge to transplantation, it is not currently approved as destination therapy. Finally, palliative and hospice level care are playing increasingly important roles in the care of stage D heart failure patients for whom the just-mentioned options are not practical and there are no reasonable prospects for improvement in quality or length of life. The subsequent early phase of rapid ventricular filling corresponds to the timing of the third heart sound (S3), which may be audible when filling pressures are increased (as in patients with heart failure). As the pressures in the left atrium and ventricle equalize, ventricular filling slows. Filling is then augmented at end diastole owing to atrial contraction, which generates the a wave on the left atrial pressure tracing. In atrial fibrillation, organized atrial contraction is absent and a discrete a wave is usually not evident. Ventricular pressure continues to rise at constant ventricular volume (isovolumic contraction) until it exceeds aortic pressure. After contraction, as the pressure in the left ventricle falls below the aortic pressure, ejection ceases and the aortic valve closes, generating the second heart sound (S2). The v waves on the right and left atrial pressure tracings correspond to venous return to the atria when the tricuspid and mitral valves are closed. With the development of left ventricular failure, pulmonary artery pressures rise and the pulmonic component of the second heart sound is accentuated. A systolic murmur of mitral regurgitation may also become audible owing to ventricular cavity dilatation. In such regions, irreversible damage has not occurred and ventricular function can improve with restoration of adequate blood flow through revascularization. It is thought to be caused by the generation of oxygen-derived free radicals or the transient loss of contractile filament sensitivity to calcium. Viability testing with thallium perfusion imaging, positron emission tomography, or dobutamine echocardiography can confirm whether the anterior wall is viable or permanently scarred. Heart failurerelated pleural effusions are usually bilateral, but when they are unilateral they are usually present on the right side. When hydrothorax develops, dyspnea becomes more marked because of a further reduction in vital capacity. The absence of pulmonary rales does not exclude considerable elevation of the pulmonary capillary pressure, especially in patients with chronic heart failure who may have well-developed lymphatic drainage. Hepatomegaly is often present in patients with heart failure before the development of overt peripheral edema. When it develops rapidly with acute congestion, the liver may be tender as a result of rapid capsular distention. Peripheral edema often does not correlate well with the degree of systemic venous congestion. The exclusion of thinned, scarred myocardium restores an elliptical shape to the left ventricle with the goal of diminishing wall stress, mitral regurgitation, and residual ischemia. Orthopnea refers to dyspnea that develops quickly after lying in the recumbent position, relieved by sitting upright. Although common in patients with heart failure, orthopnea is a nonspecific symptom that may occur in any condition in which pulmonary vital capacity is decreased, such as ascites, a large pleural effusion, or obstructive lung disease. In severe heart failure, the stroke volume is reduced and is reflected by a reduced pulse pressure. Pulsus alternans is characterized by a regular heart rhythm with an alternating strong and weak peripheral pulse. It signifies advanced myocardial disease and is likely due to cyclical alteration in the left ventricular stroke volume due to incomplete myocardial recovery after contraction. Heart failure with preserved ejection fraction ("diastolic heart failure") occurs most commonly in patients who are elderly, female, and hypertensive. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): Developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart Rhythm Society. Side effects can be minimized by maintaining therapeutic levels of digoxin between 0. Digitalis toxicity may be manifest by neurologic symptoms (visual abnormalities, confusion), gastrointestinal disturbance (nausea, vomiting), or ventricular or supraventricular tachycardias and bradyarrhythmias. Conversely, direct-current cardioversion can precipitate serious ventricular arrhythmias in patients with overt digitalis toxicity and elective cardioversion should be avoided. Owing to its significant binding to plasma proteins and its large volume of distribution, digoxin is not efficiently removed by dialysis. However, in cases of lifethreatening overdose, antidigoxin immunotherapy can prove lifesaving. Doses of purified antidigoxin Fab are administered on the basis of estimated dose of digoxin ingested, or total body burden. Although rare, recurrence of toxicity can occur, usually 24 to 48 hours after administration of antidigoxin immunotherapy. Owan T, Hodge D, Herges D, et al: Heart failure with preserved ejection fraction: Trends in prevalence and outcomes. Food and Drug Administration for use both as a bridge to cardiac transplantation and as permanent 120 destination therapy in patients not eligible for transplantation. Device-related infections are the second leading cause of death after cardiac failure. Bacterial pathogens dominate and are found most commonly in the blood or the percutaneous driveline. Bleeding complications may be further exacerbated by the requirement for both antiplatelet and anticoagulant therapy to prevent device-related thromboembolism. The device in the upper left chest in the radiograph is an implantable cardioverter-defibrillator. Because the left ventricular lead is typically placed over the surface of the left ventricle via a coronary sinus branch, inadvertent phrenic nerve stimulation and diaphragmatic pacing may complicate device implantation. This is in distinction to isolated right ventricular apical pacing, a mode that can contribute to dyssynchrony and a higher risk of heart failure symptoms. Such an imbalance results from (1) increased pulmonary capillary pressure, (2) decreased plasma oncotic pressure, (3) increased negativity of interstitial pressure, or (4) increased interstitial oncotic pressure. High-altitude pulmonary edema may occur in individuals who rapidly ascend to altitudes >2500 meters and then perform strenuous physical exercise before they have become acclimated. Symptoms respond quickly to descent to a lower altitude or to administration of a high inspiratory concentration of oxygen. Acute pulmonary edema may develop in women with preeclampsia or eclampsia, most commonly in the postpartum period. Many prescription drugs and drugs of abuse can cause lung injury or pulmonary edema. The precise mechanism is not known but may relate to an alveolarcapillary membrane leak induced by the drug. In particular, elevated jugular venous pressure and a third heart sound are each independently associated with adverse outcomes, including progression of heart failure. It signifies advanced myocardial disease and is likely the result of cyclic alteration in left ventricular stroke volume due to incomplete myocardial recovery after contraction. The presence of fever in congestive heart failure should always alert the physician to the possibility of underlying infection, pulmonary infarction, or infective endocarditis. In severe heart failure, low-grade fever may be seen as a consequence of cutaneous vasoconstriction and impairment of heat loss from sustained adrenergic nervous system activation. Sleep-disordered breathing is common in heart failure and is an independent risk factor for death and need for cardiac transplantation. Sleepdisordered breathing causes recurrent apnea-related hypoxemia and sleep arousal, contributing to chronic neurohormonal activation, peripheral vasoconstriction, and reduced cardiac performance. In zone 1 (at the apex), the alveolar pressure exceeds both pulmonary arterial and pulmonary venous pressures, so that there is ventilation without perfusion (dead space). In zone 2, alveolar pressure exceeds the venous but not the arterial pressure at some stage of the respiratory cycle. In zone 3, the alveolar pressure does not exceed either arterial or venous pressures. Zone 3 alveoli are therefore the best perfused and in the upright patient are situated in the dependent areas of the lung. Measurement of the pulmonary capillary wedge pressure using a balloon-tipped catheter will be misleading if the catheter tip is wedged in a zone 1 or zone 2 arterial branch. In these zones, the wedge pressure measures alveolar pressure rather than the true left atrial pressure. As a consequence, cardiomegaly is common in patients with heart failure and reduced systolic function. However, many patients develop heart failure without apparent systolic dysfunction. This group of patients with heart failure and preserved ejection fraction comprises a diverse group of patients with primary diastolic heart failure, pericardial disease, valvular heart disease, hypertrophic heart disease, or primary restrictive cardiomyopathy. A clue to identifying these syndromes is the presence of signs and symptoms of heart failure in the absence of cardiomegaly. Pulmonary vascular redistribution on the chest radiograph reflects a relative reduction of perfusion of the bases and a relative increase in apical perfusion. This phenomenon is likely due to compression of vessels at the lung bases owing to dependent edema in that zone. However, milrinone use has not been shown to improve hospital mortality rates and can be associated with hypotension, arrhythmias, and myocardial ischemia and should be used only for patients who do not respond to diuretics and noninotropic vasodilators. Vasopressin levels are elevated in both acute and chronic heart failure and are thought to be a major contributor to hyponatremia, an adverse prognostic marker.
Cost of synthroid. One Step Pregnancy Dipstick Test.
References
- Dupont FW, Lang RM, Drum ML, et al. Is there a longterm predictive value of intraoperative low-dose dobutamine echocardiography in patients who have coronary artery bypass graft surgery with cardiopulmonary bypass? Anesth Analg 2002; 95:517-523.
- Broderick GA, Arger P: Duplex Doppler ultrasonography: noninvasive assessment of penile anatomy and function, Semin Roentgenol 28(1):43n56, 1993.
- Ukimura, O., Gill, I.S. Imaging-assisted endoscopic surgery: Cleveland Clinic experience. J Endourol 2008;22:803-810.
- Haan JC, Buffart TE, Eijk PP, et al. Small bowel adenocarcinoma copy number profiles are more closely related to colorectal than to gastric cancers. Ann Oncol 2012;23(2):367-374.
- Gross CW, Becker DG, Lindsey WH, et al. The soft-tissue shaving procedure for removal of adipose tissue. A new, less traumatic approach than liposuction. Arch Otolaryngol Head Neck Surg. 1995;121(10):1117-20.
- Fernandez-Torron R, Arocha J, Lopez-Picazo JM, et al. Isolated dysphagia due to paraneoplastic myasthenic syndrome with anti-P/Q voltage-gated calcium-channel and anti-acetylcholine receptor antibodies. Neuromuscul Disord. 2011;21:126-128.